fetching data ... 
Background: Achieving complete response (CR) is a major goal in lupus nephritis management (LN), as it is linked to better long-term renal outcomes [1, 2]. Emerging evidence indicates that the duration of CR may be more crucial than simply achieving it [3, 4]. However, available data remain limited, and there is significant variation in how sustained remission is defined across studies.
Objectives: We aimed to examine the prevalence and duration of sustained CR (sCR) in an inception cohort of patients with biopsy-proven LN followed in two academic centres, and identify factors associated with its achievement. We also evaluated the impact of sCR on renal flares, severe kidney function loss [≥30% reduction in eGFR at the last follow-up visit compared to baseline], organ damage measured using the SLICC/ACR Damage Index (SDI) and overall survival, and determine the minimum duration of sCR required for a favorable long-term prognosis.
Methods: Longitudinal data from 142 patients with LN [71% proliferative (PLN), 29% membranous (MLN)], with a median follow-up of 121 (IQR: 90) months were analyzed using linear, logistic and Cox regression models. CR was defined according to the 2012 EULAR/ERA-EDTA guidelines [5] and 2021 KDIGO recommendations [6], with sCR defined as CR maintained for at least 12 consecutive months. The time to achieve sCR was measured from LN diagnosis. A composite unfavorable outcome of progression to end-stage kidney disease (ESKD) or death was defined, due to the small number of these events in the cohort.
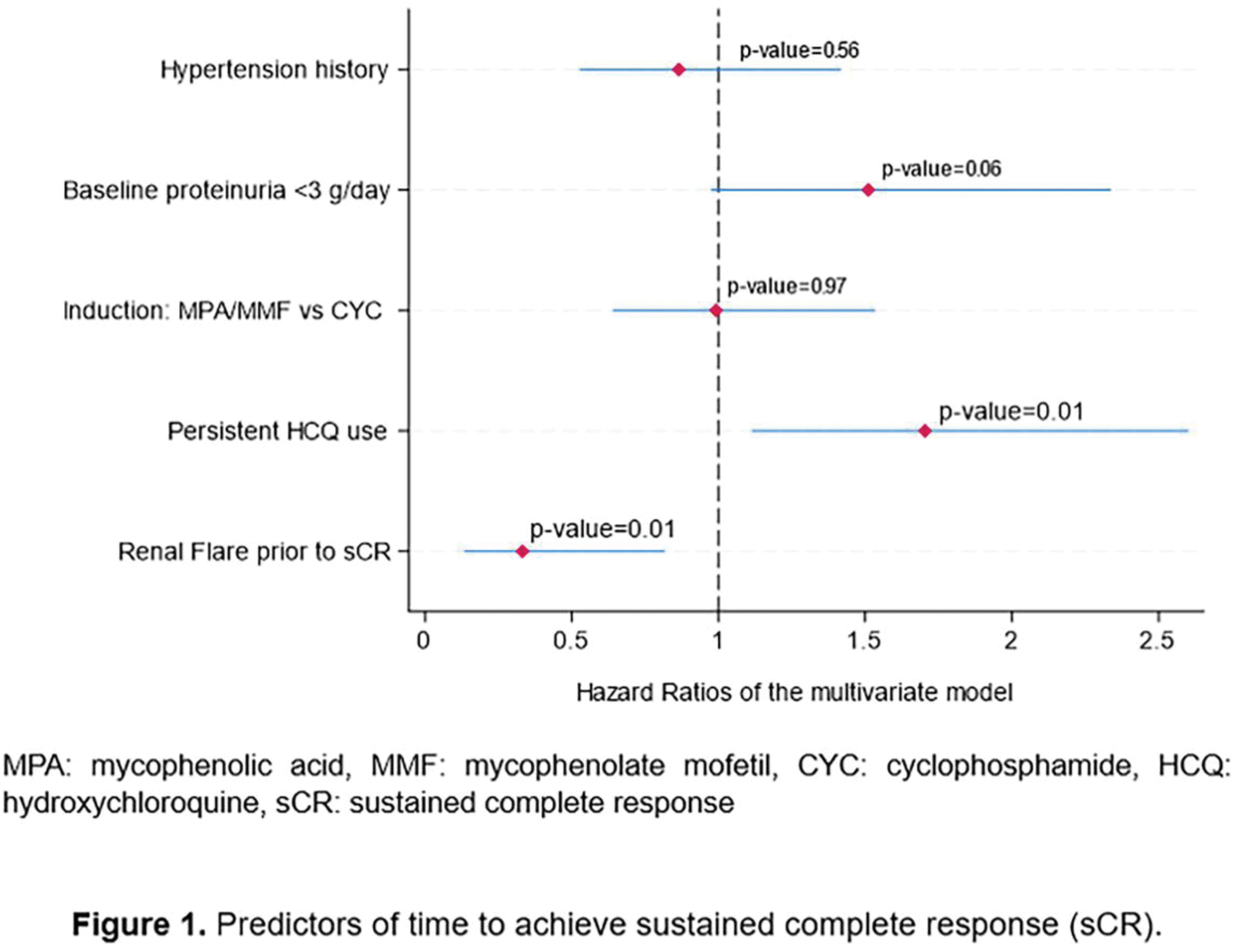
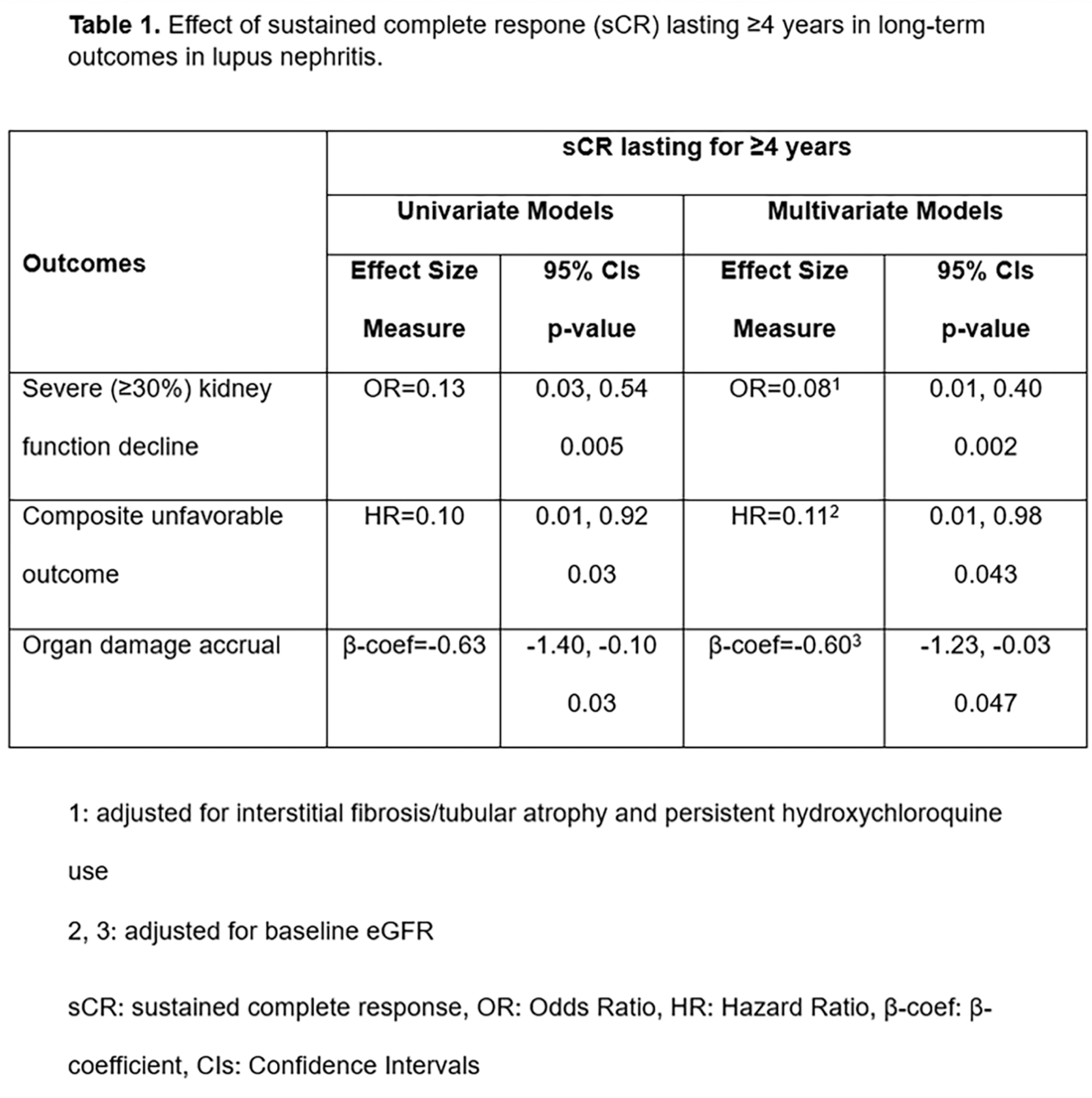
Results: In total, 118 patients (83%) achieved sCR, and 56.3% and 20.4% of them maintained it for at least 5 and 10 years, respectively. The median time to achieve sCR was 20 (IQR: 9) months post-LN diagnosis. Non-achievers of sCR were less likely to have received maintenance therapy with mycophenolic acid derivatives compared to achievers (52% vs. 74%, p=0.01) and they had a slightly lower baseline eGFR (99 vs 82.5 ml/min, p=0.09), and more severe interstitial fibrosis/tubular atrophy (20.8% vs 8.8%, p=0.08). Persistent hydroxychloroquine (HCQ) use (≥2/3 of the follow-up) (adjusted HR: 1.70, p=0.014) and absence of renal flares (adjusted HR: 0.33, p=0.016) were independently associated with a shorter time to achieve sCR, whereas there was a trend for non-nephrotic levels of baseline proteinuria (adjusted HR: 1.51, p=0.064) (Figure 1). Subgroup analysis among patients with PLN revealed similar results, with non-nephrotic proteinuria reaching statistical significance (adjusted HR: 2.30, p=0.01). Post-sCR renal flares occurred in 44 patients (37.3%), in a median time of 43.5 months (IQR: 43.5) following CR. The risk of renal flares 5 and 10 years after achieving sCR was 20% and 26.2%, respectively. Notably, the risk of flares decreased progressively with each additional year of sCR. The duration of sCR, rather than its mere achievement, was also a significant predictor of preserved kidney function (adjusted OR: 0.81, p=0.015) and improved overall survival (adjusted HR: 0.75, p=0.001) during follow-up, while achieving sCR was a strong predictor of reduced organ damage (adjusted β-coef=-1.08, p<0.001). Among patients with extended follow-up (≥100 months), the minimum sCR duration required to protect against several unfavorable outcomes was four years (Table 1). Those who achieved sCR≥4 years, had similar probability to have discontinued the immunosuppressive (IS) treatment (74% vs 78%, p=0.71) and had spent similar time on glucocorticoids (GC) (31 vs 34 months, p=0.96) compared to those who did not achieve it.
Conclusion: Achievement of sCR is feasible in a real-world setting and provides substantial benefits in terms of renal survival and damage accrual. Non-nephrotic levels of baseline proteinuria, persistent HCQ use and absence of flares are associated with shorter time to achieve sCR while four years emerged as the minimum CR duration required to protect against an unfavorable long-term prognosis.
REFERENCES: [1] Kapsia E, Marinaki S, Michelakis I, Liapis G, Sfikakis PP, Boletis J, Tektonidou MG. Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort. J Clin Med. 2022;11(17):5017.
[2] Fanouriakis A, Kostopoulou M, Cheema K, Anders HJ, Aringer M, Bajema I, et al. 2019 Update of the Joint European League against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis. Ann Rheum Dis. 2020;79:S713–23.
[3] Gatto M, Frontini G, Calatroni M, Reggiani F, Depascale R, Cruciani C, et al. Effect of Sustained Clinical Remission on the Risk of Lupus Flares and Impaired Kidney Function in Patients With Lupus Nephritis. Kidney Int Rep. 2024;9:1047–56.
[4] Pakchotanon R, Gladman DD, Su J, Urowitz MB. Sustained complete renal remission is a predictor of reduced mortality, chronic kidney disease and end-stage renal disease in lupus nephritis. Lupus. 2018;27:468–74.
[5] Bertsias GK, Tektonidou M, Amoura Z, Aringer M, Bajema I, Berden JHM, et al. Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann Rheum Dis. 2012;71:1771–82.
[6] Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4S):S1-S276.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (