fetching data ... 
Background: Bimekizumab (BKZ) is a monoclonal IgG1 antibody that selectively inhibits interleukin (IL)-17F in addition to IL-17A. BKZ has demonstrated consistent and sustained efficacy to 2 years in patients with non-radiographic (nr-) and radiographic (r-) axial spondyloarthritis (axSpA) in the parallel phase 3 studies BE MOBILE 1 and 2, respectively, and their combined open-label extension (OLE), and to 5 years in the phase 2b BE AGILE study in patients with r-axSpA [1–3].
Objectives: To assess the 3-year efficacy and safety of BKZ across the full disease spectrum of axSpA.
Methods: BE MOBILE 1 (nr-axSpA; NCT03928704) and BE MOBILE 2 (r-axSpA; NCT03928743) each comprised a 16-week, double-blind, placebo-controlled period and a 36-week maintenance period [4]. All patients received subcutaneous BKZ 160 mg every 4 weeks (Q4W) from Week 16; eligible patients could enter the OLE (BE MOVING; NCT04436640) at Week 52. Efficacy outcomes are reported for patients with nr-axSpA and r-axSpA from BE MOBILE 1 and 2 and their combined OLE up to 3 years (164 weeks [112-week OLE]; N=586). Binary outcomes were assessed using modified non-responder imputation (mNRI), continuous outcomes using multiple imputation (MI) and additional analyses using observed case (OC). mNRI considered all visits following discontinuation due to adverse events or lack of efficacy as non-response; all other missing data were imputed with MI and the response derived from the imputed values. Data were reported for the randomised set; patients not enrolled in the OLE were imputed as non-responders. MRI outcomes were assessed in the subset of patients in the MRI sub-studies. At baseline and Weeks 52, 104 and 164, MRI inflammation was evaluated using Spondyloarthritis Research Consortium of Canada (SPARCC) SIJ score (nr-axSpA only) and Berlin spine score (r-axSpA only), with readers blinded to timepoint. Pooled safety data were reported to 3 years for all patients who received ≥1 BKZ dose (N=574; exposure: 1,664.7 patient-years [PY]).
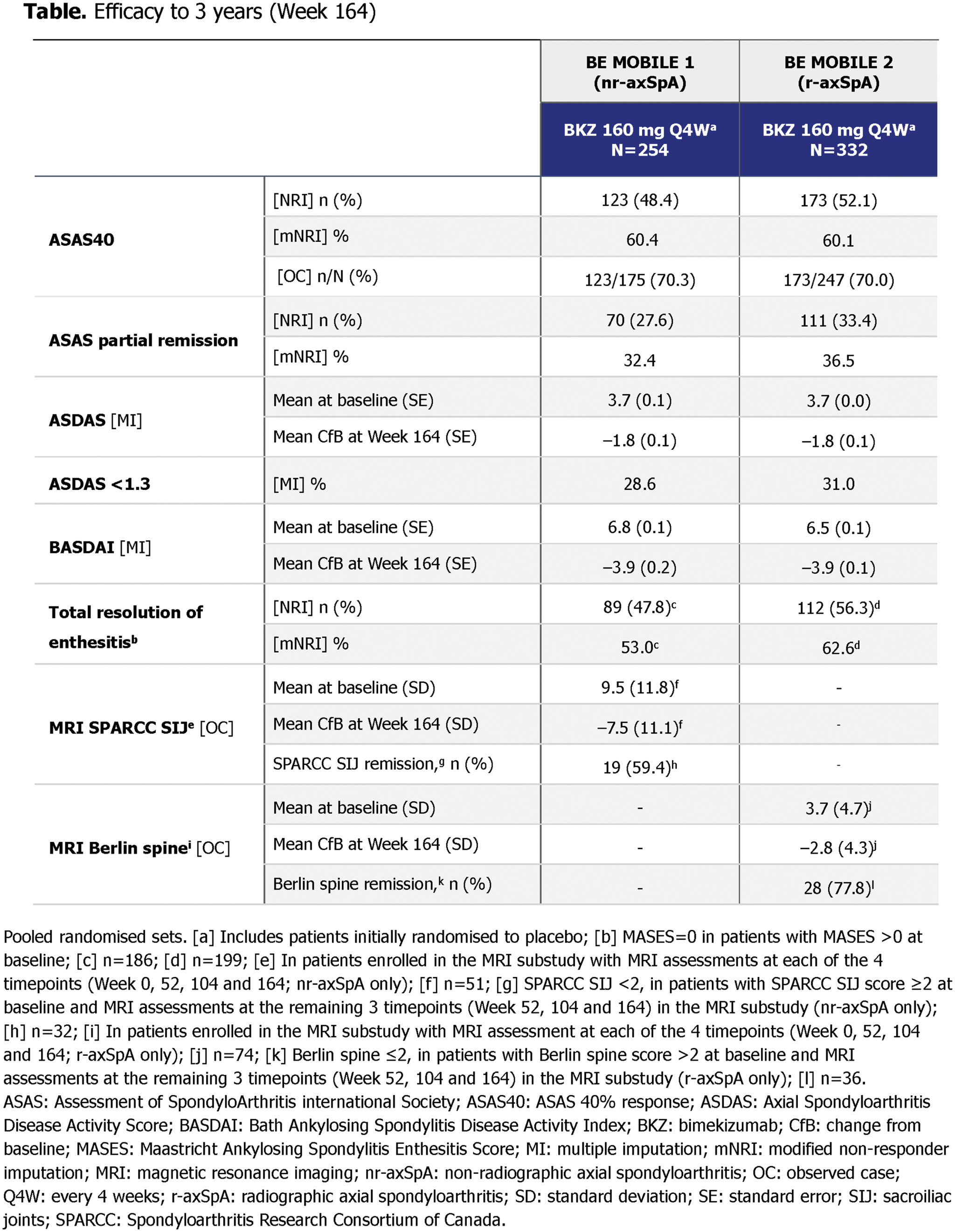
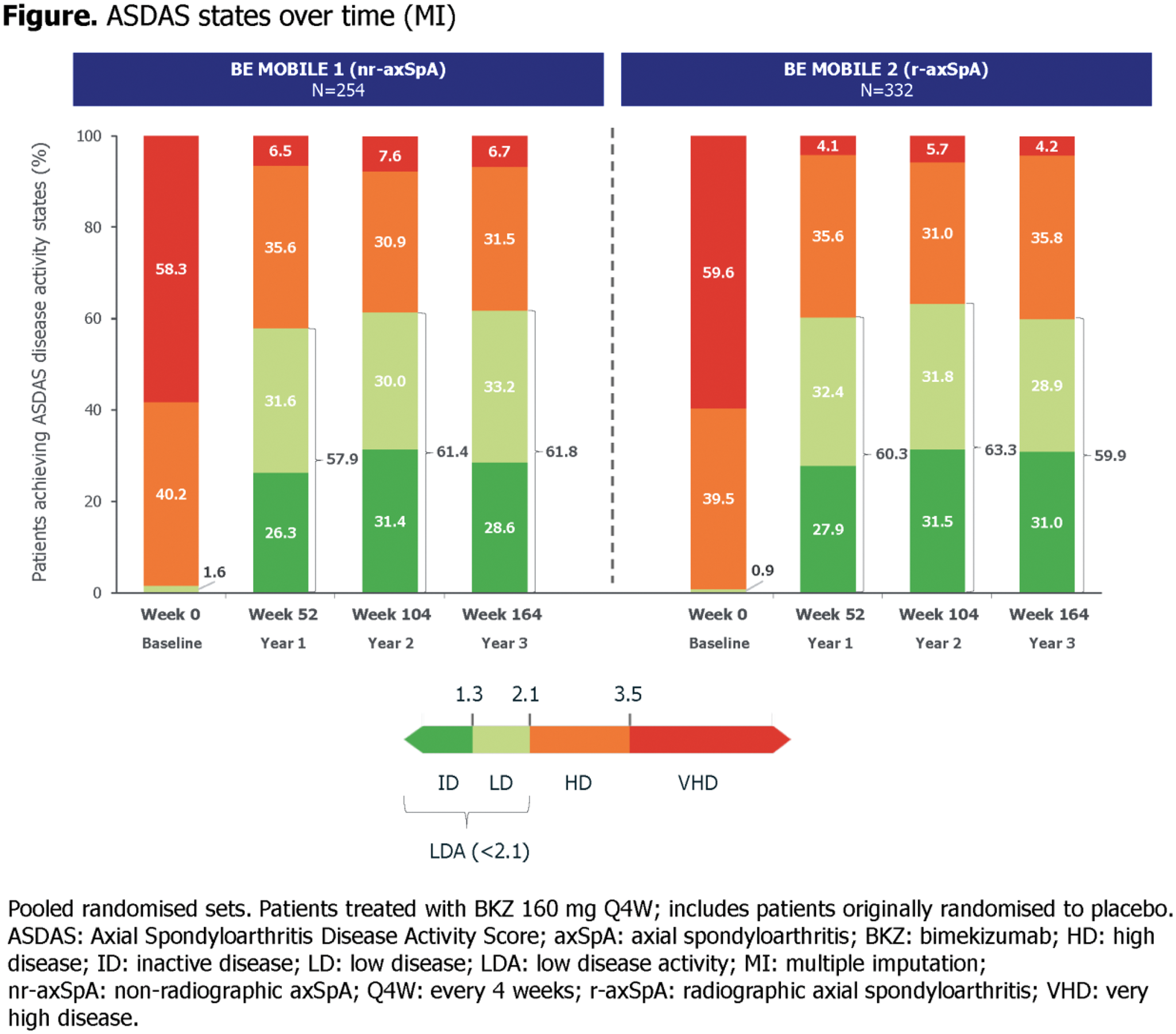
Results: Of 586 randomised patients ( nr-axSpA : 254; r-axSpA : 332), 494 (84.3%) patients entered the OLE at Week 52, with 425/494 (86.0%) completing Week 164 ( nr-axSpA : 175; r-axSpA : 250). Efficacy was sustained from 2 years to 3 years across nr-axSpA and r-axSpA populations (Figure 1; Table 1) [1]. Assessment of SpondyloArthritis international Society 40% (ASAS40) responses were maintained from Week 104 to Week 164 (mNRI; nr-axSpA : 59.4% to 60.4%; r-axSpA : 60.7% to 60.1%). At Week 164, Axial Spondyloarthritis Disease Activity Score (ASDAS) low disease activity (LDA; <2.1) was achieved by 61.8% of patients with nr-axSpA and 59.9% of patients with r-axSpA (MI). ASDAS inactive disease (ID; <1.3) and ASAS partial remission were achieved at Week 104 and Week 164 respectively by approximately a third of patients (ASDAS <1.3 [MI]: nr-axSpA : 31.4% and 28.6%; r-axSpA : 31.5% and 31.0%; ASAS partial remission [mNRI]: nr-axSpA : 34.7% and 32.4%; r-axSpA : 34.6% and 36.5%). BKZ treatment led to sustained suppression of MRI inflammation from Week 104 to Week 164, demonstrated by reductions from baseline in SPARCC SIJ (–7.4 and –7.5; nr-axSpA only) and Berlin spine scores (–2.6 and –2.8; r-axSpA only). At Week 164, >59% patients achieved MRI remission (SPARCC SIJ <2 or Berlin spine ≤2 in patients with MRI inflammation at baseline; Table 1). To Week 164, 90.4% (519/574) patients with axSpA had ≥1 treatment-emergent adverse event (TEAE) on BKZ; similar to Week 104, the most frequent TEAEs by preferred term (exposure-adjusted incidence rate per 100 PY [EAIR/100 PY]; MedDRA v19.0) were SARS-CoV-2 (COVID-19) infection (14.5), nasopharyngitis (9.9) and upper respiratory tract infection (5.8). EAIR/100 PY of serious TEAEs remained low (4.9). TEAEs leading to discontinuation of BKZ occurred in 42 patients (7.3%; EAIR/100 PY: 2.5). No deaths or adjudicated major adverse cardiovascular events were reported. Hepatic events occurred in 74 patients (12.9%; EAIR/100 PY: 4.9); all were non-serious, and the majority were transient liver function test elevations or abnormalities; none led to permanent treatment discontinuation. EAIR/100 PY was low for malignancies (0.5) and serious infections (1.2), and very low for suicidal ideation and behaviour (0.1). Of the 131 (22.8%; EAIR/100 PY: 9.4) patients who had fungal infections, 80 had Candida infections (13.9%; EAIR/100 PY: 5.3). Almost all Candida infections were mucocutaneous and mild/moderate, with one case each of severe oral and severe oesophageal infection; none were serious or systemic. Candida infections led to study discontinuation in 6/80 patients (oral [n=5] and oesophageal [n=1]). Oral candidiasis occurred in 66 patients (11.5%; EAIR/100 PY: 4.3). Incidence of uveitis (EAIR/100 PY: 1.5) and inflammatory bowel disease (EAIR/100 PY: 0.5) was low. No new safety signals were observed from Week 104 to Week 164; most EAIRs of TEAEs were similar between these timepoints.
Conclusion: BKZ demonstrated sustained clinical response through 3 years across nr-axSpA and r-axSpA, with most patients achieving ASAS40 and low disease activity. No new safety signals were observed; BKZ was well tolerated with a favourable safety profile. These results support BKZ as a durable long-term treatment option across the full disease spectrum of axSpA.
REFERENCES: [1] Baraliakos X. EULAR 2024 [POS0806].
[2] Deodhar A. ACR 2023 [0519].
[3] Baraliakos X. Ann Rheum Dis 2024;83:199–213.
[4] van der Heijde D. Ann Rheum Dis 2023;82:515–26.
Acknowledgements: Funded by UCB. Medical writing support provided by Costello Medical and funded by UCB.
Disclosure of Interests: Xenofon Baraliakos Paid instructor for AbbVie, BMS, Chugai, Eli Lilly, Galapagos, MSD, Novartis, Pfizer and UCB, Speakers bureau from AbbVie, BMS, Chugai, Eli Lilly, Galapagos, MSD, Novartis, Pfizer and UCB, Consultant of AbbVie, BMS, Chugai, Eli Lilly, Galapagos, Gilead, Novartis, Pfizer and UCB, Grant/research support from AbbVie, Celltrion, Janssen and Novartis, Atul Deodhar Speaker for Eli Lilly, J&J, Novartis, Pfizer and UCB, Consultant for BMS, Eli Lilly, J&J, MoonLake, Novartis, Pfizer and UCB, Grant/research support from BMS, Eli Lilly, J&J, Novartis, Pfizer and UCB, Désirée van der Heijde Associate editor Annals Rheumatic Diseases, editorial board member Journal of Rheumatology and RMD Open, Advisor Assessment Axial Spondyloarthritis international Society and director of Imaging Rheumatology BV, Consultant for AbbVie, Alfasigma, ArgenX, BMS, Eli Lilly, GreyWolf Therapeutics, Janssen, Novartis, Pfizer, Takeda and UCB, Filip van den Bosch Speakers bureau fees from AbbVie, Amgen, Janssen, Merck, Novartis, Pfizer and UCB, Consultancy fees from AbbVie, Alfasigma, Amgen, Eli Lilly, GreyWolf Therapeutics, Janssen, Novartis, Pfizer and UCB, Marina Magrey Consultancy fees from AbbVie, BMS, Eli Lilly, Novartis, Pfizer and UCB, Research grants from AbbVie, BMS and UCB, Walter P Maksymowych Honoraria/consulting fees from AbbVie, BMS, Boehringer-Ingelheim, Celgene, Eli Lilly, Galapagos, Janssen, Novartis, Pfizer and UCB, Research grants from AbbVie, Galapagos, Pfizer and UCB; educational grants from AbbVie, Janssen, Novartis and Pfizer, Chief Medical Officer for CARE ARTHRITIS, Tetsuya Tomita Speaker fees from AbbVie, Astellas, BMS, Eisai, Eli Lilly, Janssen, Kyowa Kirin, Mitsubishi-Tanabe, Novartis and Pfizer, Consultancy fees from AbbVie, Eli Lilly, Gilead, Novartis and Pfizer, Huji Xu Speaker for AbbVie, Janssen, Novartis, Pfizer and UCB, Consultant for AbbVie, Beigene, BioMap, IASO, Pfizer and UCB, Clinical investigator for Peking-Tsinghua Center for Life Sciences, Diana Voiniciuc Contractor for UCB and employee of Veramed, Chetan Prajapati Contractor for UCB and employee of Veramed, Myriam Manente Shareholder of UCB, Employee of UCB, Alexander Marten Employee of UCB, Lianne S Gensler Consulting fees from Acelyrin, Eli Lilly, Janssen, Novartis, Pfizer and UCB, Grants from UCB paid to institution.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (