fetching data ... 
Background: Patients with systemic lupus erythematous (SLE) have an increased bone fragility and increased fracture risk and this is thought to be related with inflammation and high disease activity but also due to therapeutic options, namely corticosteroids. SLE classically affects premenopausal women and represents per se a risk for earlier morbidity and mortality in this young population. Clarifying the features that influence fracture incidence in SLE patients other than the well-known fracture risk factors is essential to attain effective fracture prevention strategies in this population.
Objectives: To study the prevalence and risk factors for fractures in a portuguese population with SLE.
Methods: Retrospective single-center study including patients with SLE diagnosis according to the 2019 EULAR/ACR classification criteria extracted from Reuma.pt/SLE (the Portuguese national registry). Patients were excluded if they were lost to follow-up for reasons other than death. Vertebral radiographies and clinical registries were reviewed to assess the occurrence of fractures. The outcome of fractures was compared using Kaplan-Meier with the log rank test and cox regression with univariate and multivariate models adjusting for covariates.
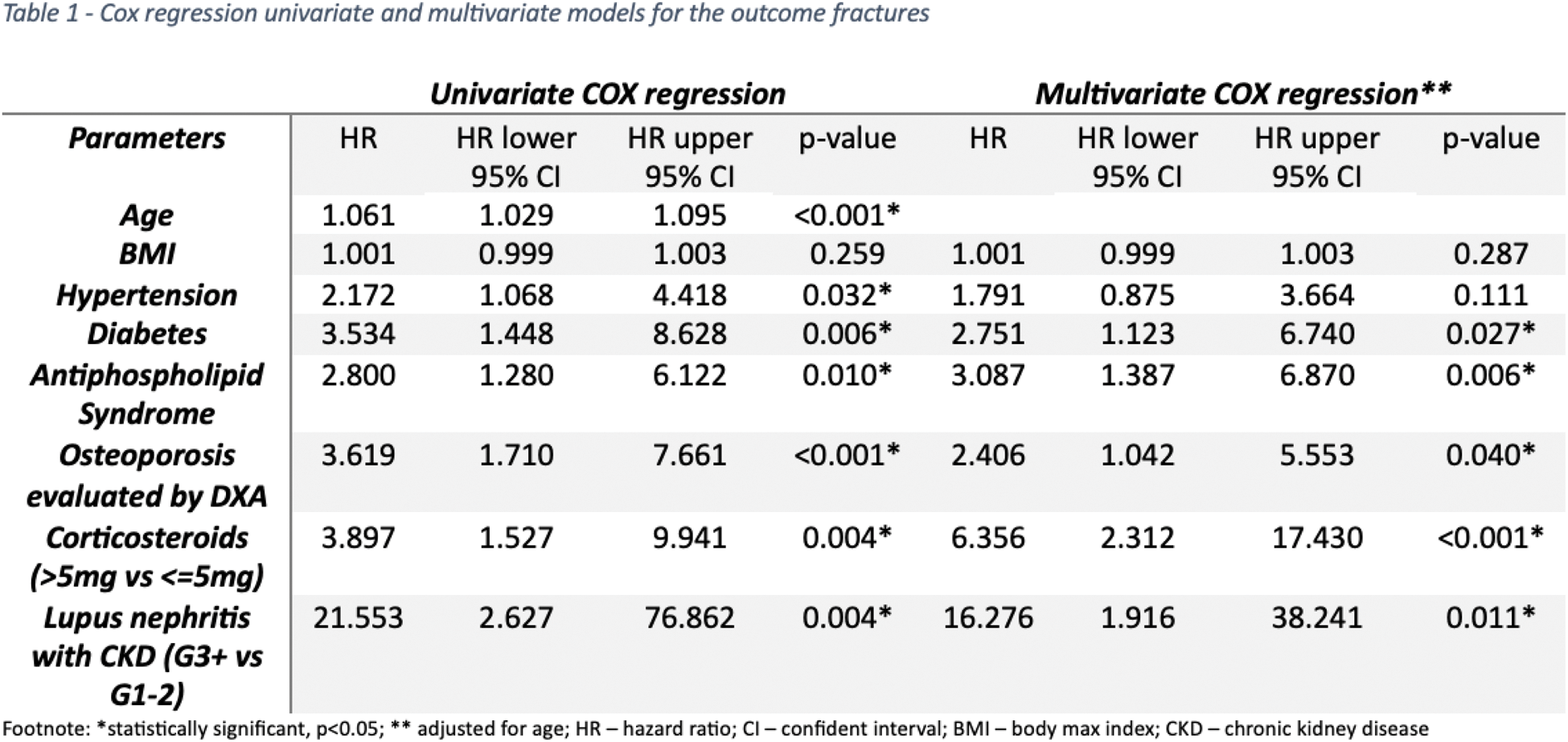
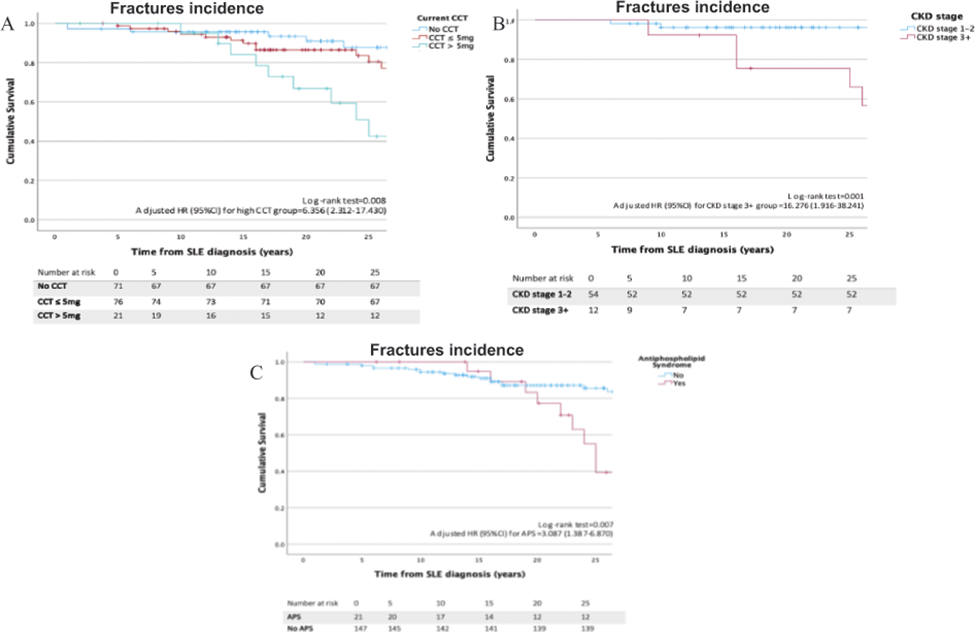
Results: A total of 170 patients with SLE were included, mostly female (n=156, 75%). Mean age at diagnosis was 32.1±13.5 years old, median follow-up time was 22 (15.4-30.2) years, and the mean current age was 54.1 ±12.6 years old. Median body max index (BMI) was 25.7 (21.9-29.3) kg/m2. Current corticosteroid dosage was 2.5 (0-5.0) mg prednisolone equivalent, 84 (49.4%) patients were currently taking conventional synthetic disease modifying antirheumatic drugs (csDMARDs) and 24 (14.1%) biologic DMARDs. A total of 71 patients (34.1%) were no longer under corticosteroids. Fractures occurred in a total of 33 patients (15.9%) including 17 (8.2%) clinical evident fractures and 24 (11.5%) asymptomatic vertebral fractures. Twenty-three patients (11.1%) had osteoporosis according to bone mineral density (BMD) assessed with dual-x ray absorptiometry (DXA) and 30 (17.6%) were under anti-osteoporotic treatment, mainly with oral or intravenous (IV) biphosphonates (56.7%, n=17). Patients who sustained fractures were older (63.1±9.7 vs 51.9±12.2, p=<0.001), had a higher BMI (27.1 vs 26.0, p=0.038) and had more frequent hypertension (p=0.003), diabetes (p=0.011) and antiphospholipid syndrome (p=0.017). As expected, most women with fractures were post-menopausal (n=26, 81.3%). The current corticosteroids dosage was higher in patients with fractures (5, 3.1-6.9mg vs 2.5, 0-5mg, p=<0.001) and a minority of patients were without corticotherapy in this group (27.3% vs 45.3%, p=0.014). The occurrence of major cardiovascular events (24.2% vs 10.9%, p=0.048) and death (27.3% vs 8.8%) were also more prevalent in the fractures group. Amongst patients with renal involvement, a chronic kidney disease (CKD) stage ≥ 3 was associated with fractures incidence (87.5% vs 11.7%, p<0.001). There were no differences regarding other clinical or immunological features and biologic or csDMARDs options in the patients who sustained fractures. In the survival analysis, patients under a corticosteroids dosage (prednisolone equivalent) > 5mg, lupus nephritis with CKD stage ≥3 and patients with associated antiphospholipid syndrome had a significantly higher incidence of fractures during follow-up (Figure 1). When adjusting for current age, lupus nephritis CKD stage ≥ 3 (HR 16.276 CI 95% 1.916-38.241, p=0.011), a corticosteroids dosage > 5mg (HR 6.356 CI 95% 2.312-17.430, p=<0.001), the presence of osteoporosis evaluated by DXA (HR 2.406 CI 95% 1.042-5.553, p=0.040) and antiphospholipid syndrome (HR 3.087 CI 95% 1.387-6.870, p=0.006) independently predicted the occurrence of fractures during follow-up, with the greatest impact being attributed to corticosteroids and actual renal function (Table 1).
Conclusion: According to our results, SLE lupus nephritis patients with worse renal function and with concurrent antiphospholipid syndrome appear to be particularly at high-risk for fractures and may warrant an earlier and more vigilant fracture prevention strategy. Corticosteroids were still currently used in the majority of our patients and the higher incidence of fractures in the group on > 5mg/daily prednisolone emphasizes the current recommendation of aiming at the lowest dose and discontinuation when possible.
Fracture survival analysis according to (A) CCT dosage, (B) CKD stage, (C) APS presence.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: Mariana Diz Lopes: None declared, Bernardo Fernandes: None declared, Carlos Marques-Gomes: None declared, Miguel Correia Natal: None declared, Bárbara Fernandes Esteves: None declared, Mariana Sebastião: None declared, Inês Almeida: None declared, Teresa Martins-Rocha Pierre-Fabre, Miguel Bernardes Abbvie, Janssen, AstraZeneca, Pfizer, Abbvie, Jansse, AstraZeneca, GSK, Pfizer, Lúcia Costa: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (