fetching data ... 
Background: The VISIBLE Phase 3b study enrolled participants with predominant skin (Cohort A) or scalp (Cohort B) moderate to severe plaque psoriasis (PsO) across all skin tones.
Objectives: This post hoc analysis was conducted to assess efficacy and patient-reported outcomes at Week 16 for participants with psoriatic arthritis (PsA) at baseline.
Methods: Participants were randomized (3:1) to receive guselkumab (GUS) 100 mg or placebo (PBO) at Week 0, Week 4, then every 8 weeks (Q8W). PsA was identified based on history of rheumatologist-diagnosed PsA or Psoriasis Epidemiology Screening Tool (PEST) score ≥3 at screening. The physical, social, and psychological impact of PsA was assessed via the Psoriatic Arthritis Impact of Disease (PsAID-12; range, 0-10; patient-acceptable symptom score [PASS] = score ≤3.95; minimal clinically important improvement [MCII] = reduction of ≥3.0) [1, 2]. In participants with PsA and baseline Investigator’s Global Assessment (IGA) score ≥2 and PsO body surface area (BSA) ≥3%, skin improvement was assessed using IGA, Psoriasis Area and Severity Index (PASI), and BSA outcomes.
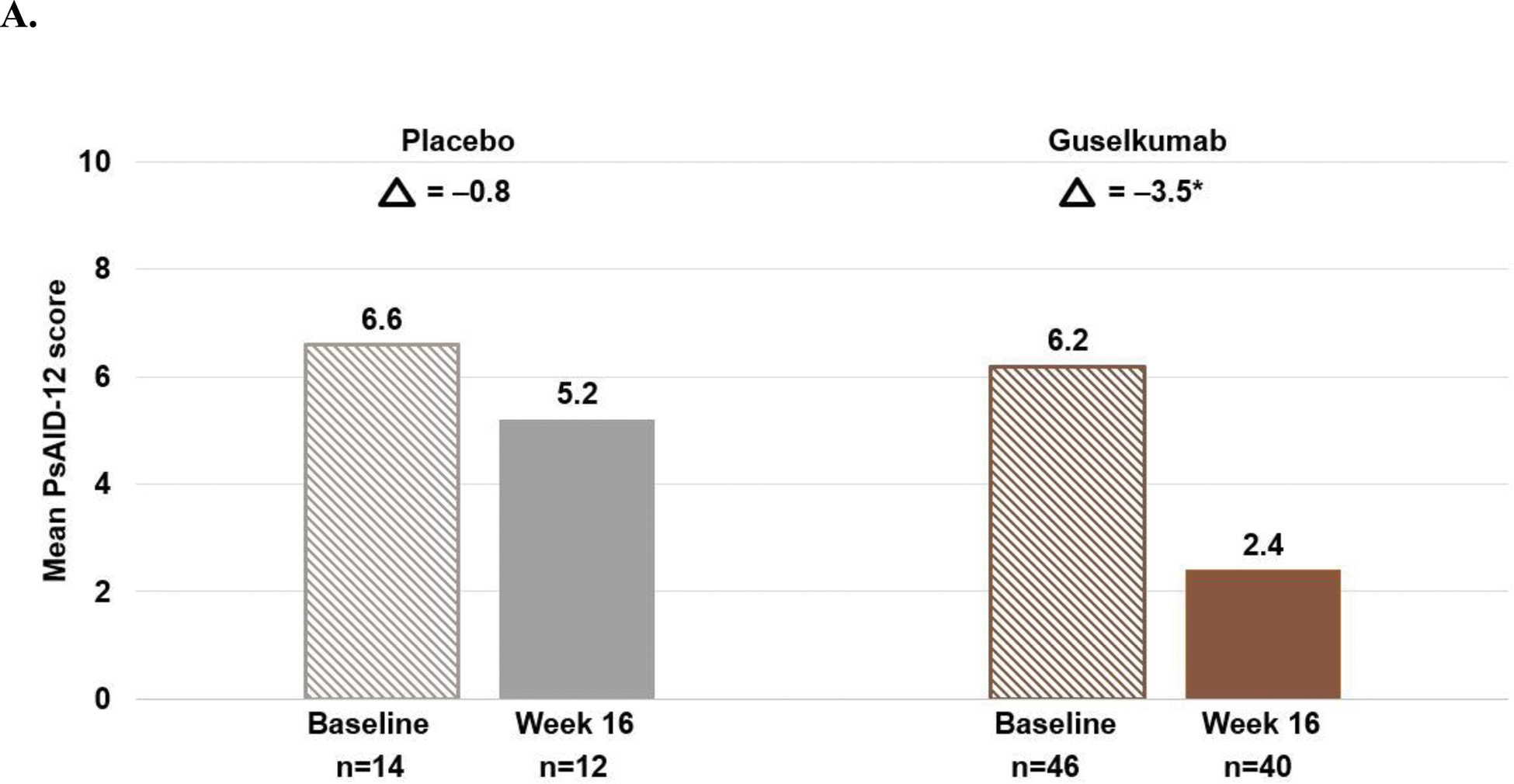
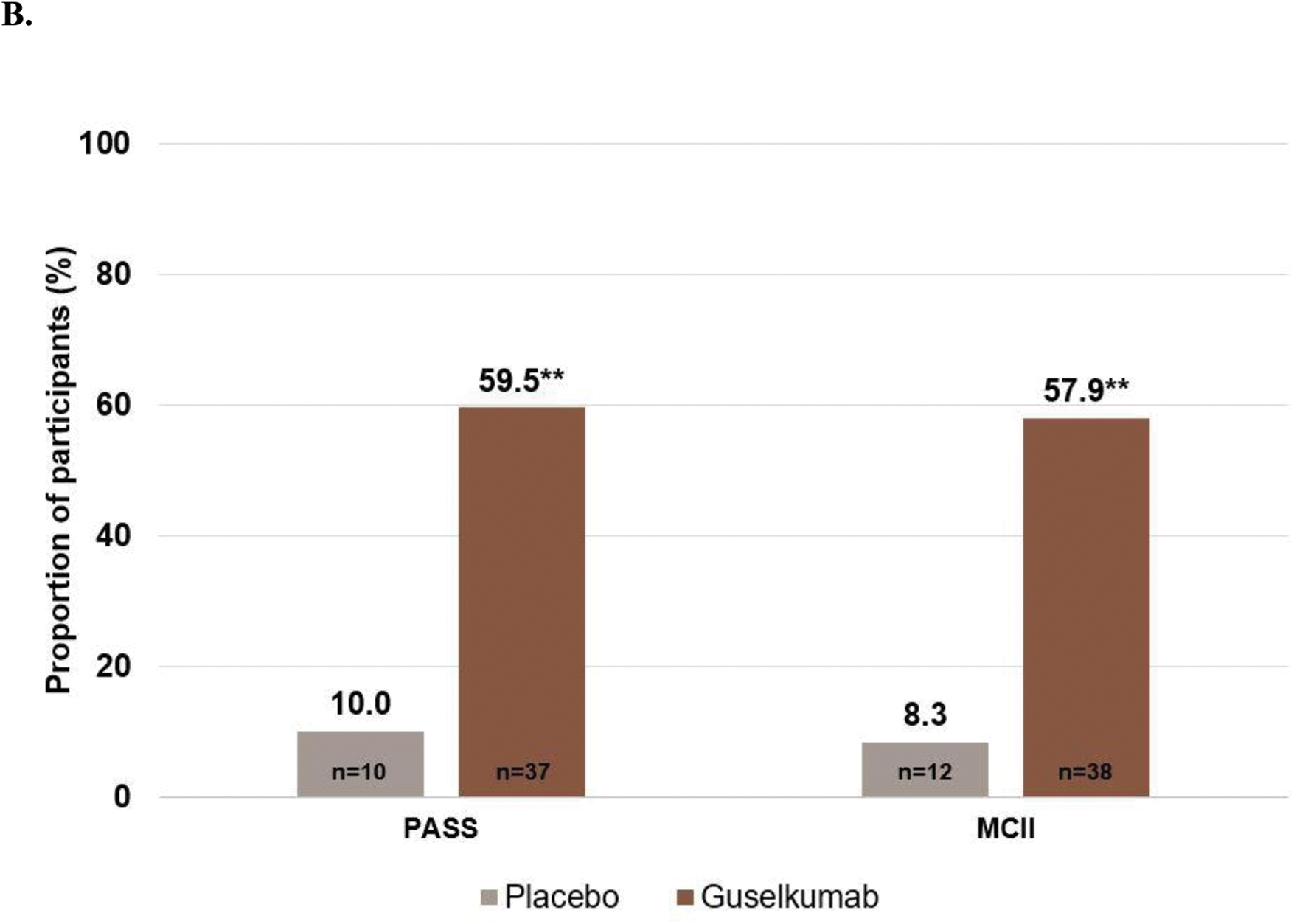
Results: Among 205 VISIBLE Cohort A and Cohort B participants, 29.8% (n=61) had PsA at baseline. Mean baseline data reflected extensive skin disease (PASI=20.0; BSA=23.6%), severe scalp PsO (Psoriasis Scalp Severity Index=28.5; scalp surface area=45.3%), and moderate impact of PsA on health (PsAID-12 score=6.2; 77.0% had baseline score >3.95). At Week 16, the least squares (LS) mean change from baseline in PsAID-12 was –3.5 with GUS vs –0.8 with PBO (nominal p<0.001; Figure 1A). Approximately 60% of GUS-treated participants with baseline PsAID-12 >3.95 and ≥3.0 achieved PASS and MCII, respectively (Figure 1B). The majority of GUS-treated participants with PsA achieved the coprimary endpoints of IGA 0/1 (72.3%) and PASI 90 (59.6%); >40% had complete skin clearance vs none in the PBO group (all nominal p<0.01). Mean percentage change in BSA from baseline at Week 16 was –84.8% with GUS vs –3.3% with PBO; mean percentage change in PASI was –86.9% with GUS vs –19.2% with PBO.
Conclusion: At baseline, the majority of VISIBLE participants with PsA had PsAID-12 scores above the PASS threshold, indicating need for improved PsA control in skin of color populations. After 3 GUS doses, ~60% of these participants achieved clinically meaningful improvements in their PsA symptoms and health-related quality of life. Consistent with the overall VISIBLE population, the majority of GUS-treated participants with PsA achieved significantly clearer skin as assessed by IGA, PASI, and BSA measures.
REFERENCES: [1] Gossec L, et al. Ann Rheum Dis . 2014;73:1012-9.
[2] Holland R, et al. J Psoriasis Psoriatic Arthritis . 2022;5:12-22.
Mean PsAID-12 scores at baseline and Week 16 (A), and achievement of PsAID-12 response thresholds at Week 16 (B).
*nominal p<0.001 vs placebo.
Δ=LS mean difference between baseline and Week 16 among participants with data at both timepoints.
LS mean differences and p-value are based on an analysis of covariance model, with treatment group, baseline PsAID-12 score, and Fitzpatrick Skin Type (I-III or IV-VI) as covariates. Participants who met treatment failure rules (discontinued study agent due to lack of efficacy, had worsening psoriasis, or initiated a prohibited psoriasis treatment prior to Week 16) were assigned a change from baseline=0. Missing data were not imputed.
LS=Least squares; PsAID-12=Psoriatic Arthritis Impact of Disease.
**nominal p≤0.01 vs placebo.
p-values are based on Fisher’s exact test. Participants meeting treatment failure criteria or with missing data were considered non-responders.
Achievement of PASS (PsAID-12 ≤3.95) was assessed for participants with PsAID-12 scores >3.95 at baseline.
Achievement of MCII (reduction of ≥3.0 points) was assessed for participants with PsAID-12 scores ≥3.0 at baseline.
MCII=Minimal clinically important improvement; PASS=Patient-acceptable symptom score; PsAID-12=Psoriatic Arthritis Impact of Disease.
Acknowledgements: NIL.
Disclosure of Interests: Alice B. Gottlieb Honoraria as an advisory board member and consultant for Amgen, AnaptypsBio, Avotres Therapeutics, Boehringer Ingelheim, Bristol Myers Squibb, Dice Therapeutics, Eli Lilly, Highlights Therapeutics, Janssen, Novartis, Sanofi, Teva, UCB, and Xbiotech (stock options for RA), Research/educational grants from Bristol Myers Squibb, Highlights Therapeutics, Janssen, and UCB Pharma (all paid to Mount Sinai School of Medicine), Amy McMichael Consultant/advisor for AbbVie, Almirall, Arcutis, Bristol Myers Squibb, Eli Lilly, Galderma, Janssen, Johnson & Johnson, L’Oréal, Nutrafol, Pfizer, Revian, Sanofi-Genzyme, UCB, Grants (funds to institution) for AbbVie, Almirall, Arcutis, Bristol Myers Squibb, Eli Lilly, Galderma, Janssen, Johnson & Johnson, L’Oréal, Nutrafol, Pfizer, Revian, Sanofi-Genzyme, UCB, Tina Bhutani Principal investigator for studies being sponsored by AbbVie, Castle, CorEvitas, Dermavant, Galderma, Mindera, and Pfizer; additional research funding from Novartis and Regeneron; advisor for AbbVie, Arcutis, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Janssen, Leo Pharma, Pfizer, Novartis, Sun, and UCB, Olivia Choi Stockholder of Johnson & Johnson, Employee of Janssen Scientific Affairs, LLC, Theodore Alkousakis Stockholder of Johnson & Johnson, Employee of Janssen Scientific Affairs, LLC, Jenny Jeyarajah Employee of Janssen Research & Development, LLC, Donna Febres Stockholder of Johnson & Johnson, Employee of Janssen Scientific Affairs, LLC, Oyediran Adelakun Stockholder of Johnson & Johnson, Employee of Janssen Scientific Affairs, LLC, Soumya D. Chakravarty Stockholder of Johnson & Johnson, Employee of Janssen Scientific Affairs, LLC, Daphne Chan Stockholder of Johnson & Johnson, Employee of Janssen Scientific Affairs, LLC, Joseph F. Merola Consultant and/or investigator for AbbVie, Amgen, AstraZeneca, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Dermavant, Eli Lilly, Incyte, Janssen, Leo Pharma, Moonlake, Novartis, Pfizer, Sanofi-Regeneron, Sun Pharma, and UCB.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (