fetching data ... 
Background: For patients with psoriatic arthritis (PsA) with an intolerance of or inadequate response to at least one conventional synthetic DMARD (csDMARD) or biological DMARD (bDMARD) like TNF inhibitors (TNFis), recent treatment guidelines from EULAR recommend switching to a JAK inhibitor (JAKi) or to another bDMARD, including cycling within the TNFi class. There is mixed evidence that cycling to another TNFi after failure of a first-line TNFi is associated with lower response rates on joint symptoms, a common feature of PsA. However, there are limited studies that investigate whether cycling to another TNFi or switching to a different mechanism of action is more favorable.
Objectives: Thus, the aim of this study was to compare the effectiveness of switching from a first-line TNFi to upadacitinib (UPA), an oral JAKi, versus cycling to another TNFi or switching from a TNFi to an IL-17 inhibitor (IL-17i) on tender and swollen joint involvement in patients with PsA.
Methods: Data were drawn from the Adelphi Real World Spondylarthritis (SpA) V and VI Disease Specific Programmes™, cross-sectional surveys administered to physicians (rheumatologists, dermatologists, and internal medicine specialists) and their consulting patients in routine clinical practice in Germany, France, Italy, Spain, the United Kingdom, and the United States (SpA VI only), with respective data collection periods from March 2021 to November 2021 for SpA V and from June 2023 to June 2024 for SpA VI. Adult patients with PsA who switched treatment from a TNFi in the first line of advanced therapy to another advanced therapy were stratified by the second-line therapy of interest: TNFi to UPA, TNFi to TNFi, or TNFi to IL-17i. The key outcome of physician-reported assessment of both TJC ≤ 1 and SJC ≤ 1 was evaluated ≥ 3 months from treatment switch. Patient demographics and clinical characteristics were balanced using inverse-probability-weighted regression adjustment (IPWRA).The covariates balanced within the IPWRA were age, sex, Charlson Comorbidity Index (CCI), and severity at initiation of second-line therapy as reported by their physician for the weighting and regression adjustment stage, and additionally second-line treatment duration was used for the regression adjustment stage. The regression analyses were conducted separately for comparisons between TNFi to UPA and TNFi to TNFi as well as between TNFi to UPA and TNFi to IL-17i.
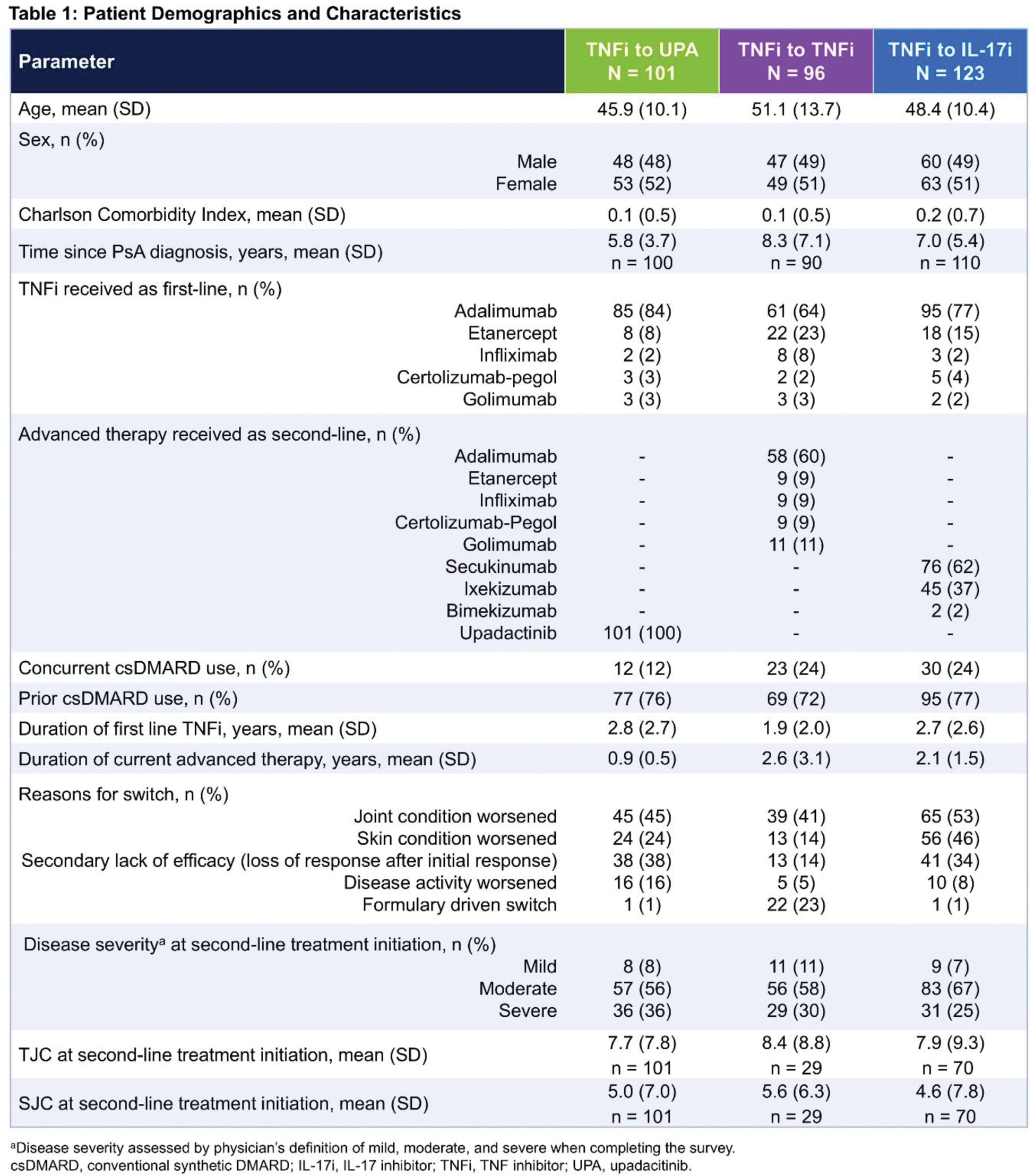
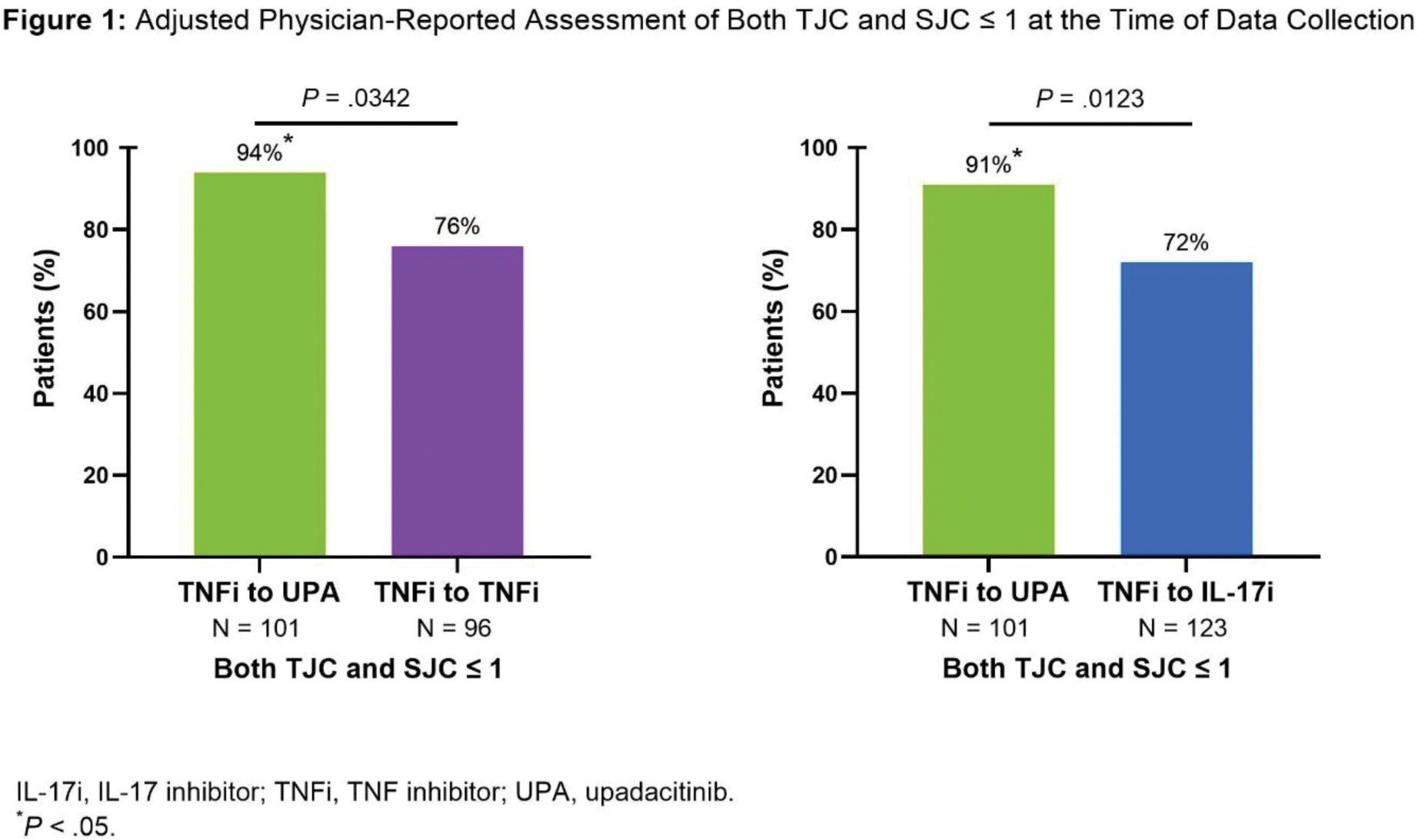
Results: Of the 320 patients included in the analysis who switched from a first-line TNFi, 101 switched to UPA, 96 switched to a second TNFi, and 123 switched to an IL-17i. Patient demographics are presented in Table 1. The most commonly used first-line TNFi in each group was adalimumab. The most commonly used second-line therapy in the TNFi to TNFi group was adalimumab while secukinumab was the most used second-line therapy in the TNFi to IL-17i group. The most frequent reason for switching reported by the physician was a worsening of the joints. At the time of switch, most patients had a physician-reported assessment of moderate/severe disease severity (TNFi to UPA: 92%; TNFi to TNFi: 89%; TNFi to IL-17i: 93%). After adjustment via IPWRA, significantly more patients in the TNFi to UPA group had physician-reported assessment of both TJC and SJC ≤ 1 at the time of data collection compared with patients in the TNFi to TNFi group (94% vs. 76%; P =.0342) and the TNFi to IL-17i group (91% vs. 72%; P =.0123) (Figure 1).
Conclusion: Patients who switched from their first TNFi advanced therapy to UPA as their second-line advanced therapy had significantly lower levels of tender and swollen joint involvement than cycling to a second TNFi or switching to an IL-17i. The results demonstrate that switching to UPA after a TNFi may benefit patients with PsA.
REFERENCES: [1] Gossec L, et al. Ann Rheum Dis. 2024;83(6):706-719.
[2] Abramson SR, et al. J Psoriasis & Psoriatic Arthritis. 2016;1(3):102-111.
Acknowledgements: Data collection was undertaken by Adelphi Real World as part of an independent survey, entitled the Spondyloarthritis (SpA) V and VI Disease Specific Programme (DSP™). The DSP is a wholly owned Adelphi product and is the intellectual property of Adelphi Real World. The analysis described here used data from the Adelphi SpA V and VI DSP. AbbVie was one of multiple subscribers to the DSP and did not influence the original survey through either contribution to the design of questionnaires or data collection. All authors had access to relevant data and participated in the drafting, review, and approval of this publication. No honoraria or payments were made for authorship. Medical writing support was provided by Kathleen E. Gordon, PhD of AbbVie. Editorial support was provided by Angela T. Hadsell AbbVie.
Disclosure of Interests: Philip J. Mease has received speakers fees from AbbVie, Acelyrin, Amgen, Bristol Myers, Inmagene, Janssen, Lilly, Moonlake, Novartis, Pfizer, and UCB, consulting fees from AbbVie, Acelyrin, Amgen, Bristol Myers, Inmagene, Janssen, Lilly, Moonlake, Novartis, Pfizer, and UCB, research grants from AbbVie, Acelyrin, Amgen, Bristol Myers, Inmagene, Janssen, Lilly, Moonlake, Novartis, Pfizer, and UCB, William Tillett has received consulting fees from AbbVie, Amgen, Celgene, Eli Lilly, GSK, Janssen, MSD, Novartis, Ono-Pharma, Pfizer, and UCB, research grants from AbbVie, Celgene, Eli Lilly, GSK, Janssen, Pfizer, and UCB, Xiaolan Ye is an employee of AbbVie and may hold stock or options, Christopher D Saffore is an employee of AbbVie and may hold stock or options, Molly Edwards is an employee of Adelphi Real World, acted as a consultant to AbbVie for this analysis, Isabel Truman is an employee of Adelphi Real World, acted as a consultant to AbbVie for this analysis, Sophie Barlow is an employee of Adelphi Real World, acted as a consultant to AbbVie for this analysis, Jayne Stigler is an employee of AbbVie and may hold stock or options, Bhumik Parikh is an employee of AbbVie and may hold stock or options, Daniel Aletaha has received speakers fees from Bristol Myers Squibb, Merck Sharp & Dohme, UCB, AbbVie, Amgen, Celgene, Eli Lilly, Medac, Merck, Novartis, Pfizer, Roche, Sandoz, and Sanofi, consulting fees from Janssen, AbbVie, Amgen, Celgene, Eli Lilly, Medac, Merck, Novartis, Pfizer, Roche, Sandoz, and Sanofi, an research grants from AbbVie, Merck Sharp & Dohme, Novartis, and Roche.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (