fetching data ... 
Background: Idiopathic inflammatory myopathies (IIM) are a heterogeneous group of diseases with an increased morbidity and mortality often due to multiorgan involvement and increased risk of infection, which can lead to hospitalization in the intensive care unit (ICU). To date, there is only limited data on the outcomes and treatments of IIM patients in the ICU.
Objectives: The aim was to analyze the clinical characteristics and outcomes of patients with IIM in the ICU to provide better insight into the management of critically ill patients with these rare diseases.
Methods: A retrospective analysis of patient charts was performed at the ICU department of the university hospital Hamburg-Eppendorf. The study was approved by the local ethics committee. ICU patients from 2014 to 2022 were screened for myositis-associated diseases (according to ICD10 codes). IIM entity, previous treatments, underlying causes of ICU admission, as well as outcomes, were analyzed.
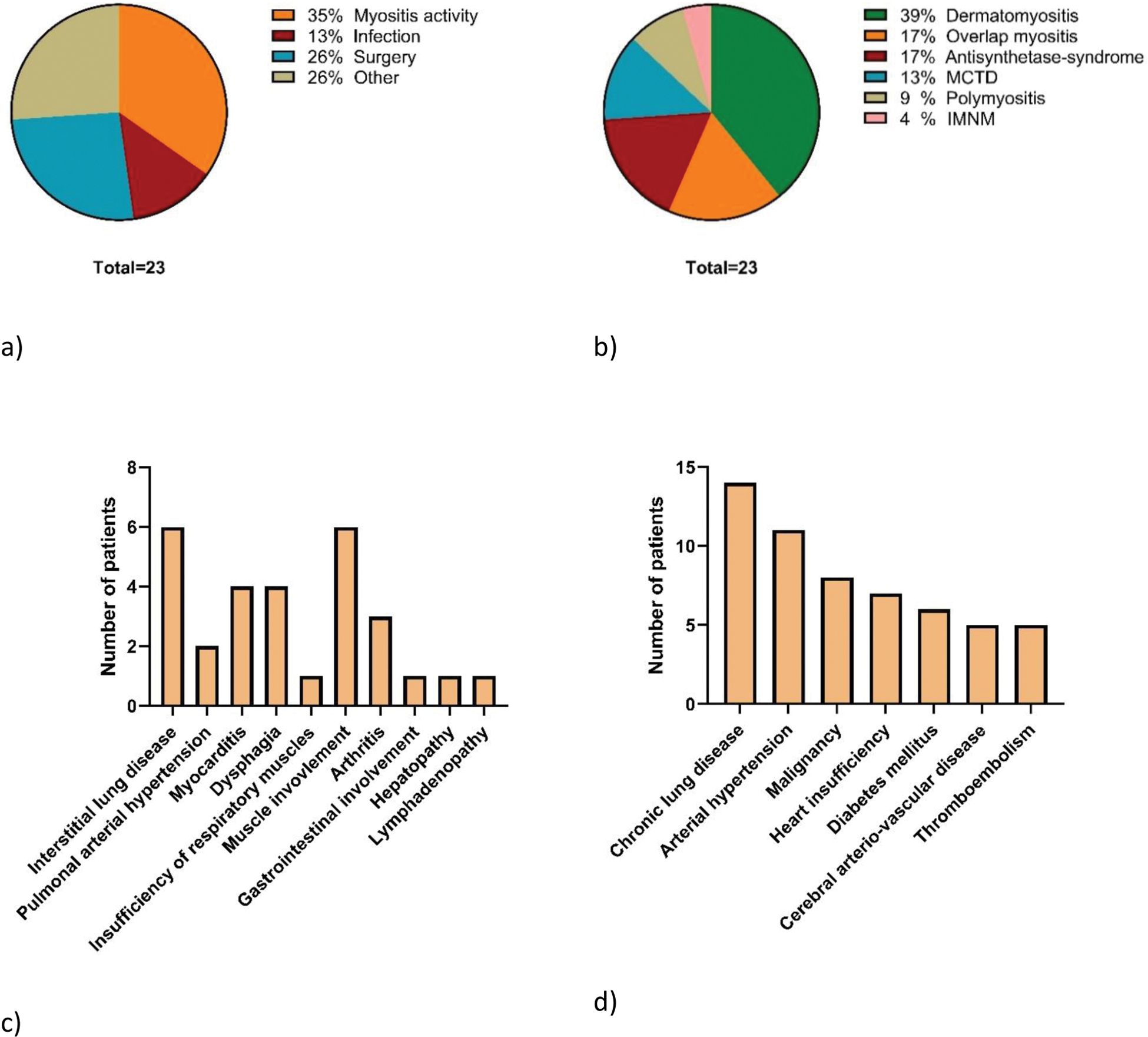
Results: Overall, 23 patients were included in the analysis, of whom 15 (65%) were female. Mean age at ICU admission was 58 years (range 19-83 years) and mean duration of ICU treatment was 32 days (range 1-503 days) (Table 1). Infectious complications under immunosuppressive therapy or IIM activity were the reason for ICU admission in almost 50% of the patients (Figure 1a). 5 (22%) patients died in the ICU (3 from bleeding complications, 2 from infectious complications) (Table 1). Most patients had dermatomyositis (39%), overlap myositis (17%) or antisynthetase-syndrome (17%) with a mean disease duration of 13 years (Table 1, Figure 1b). 14 patients had a concomitant chronic lung disease (including 10 with interstitial lung disease (ILD) and 4 cases with chronic obstructive bronchitis). Furthermore, 8 patients (35%) had a malignancy as comorbidity, 6 of whom had an active malignancy (Figure 1d). 21 patients were on immunosuppressive treatment at the time of admission (Table 1). During the ICU stay 12 patients were suffering from IIM disease activity mainly due to pulmonary, muscle and cardiac involvement (Figure 1c). In these 12 patients, immunosuppressive therapy was intensified during ICU hospitalization (glucocorticoid pulse therapy was applied in 10 patients, intravenous immunoglobulins in 6 patients, rituximab and cyclophosphamide in 3 patients, respectively). Infectious complications during ICU hospitalization were noted in 11 patients, all of whom had pulmonary infections. In addition, an abdominal infection was detected in 3 cases (Table 1). 14 patients were intubated during the ICU stay, 8 of them due to respiratory insufficiency.
Conclusion: The study gives an overview of the clinical spectrum of IIM patients admitted to the ICU. Both active disease (such as ILD or cardiac involvement) as well as infectious complications can lead to severe morbidity with a potentially life-threatening course. Associated comorbidities such as chronic lung diseases or malignancies can further predispose to poor outcomes. The combination of disease activity and infectious complications highlights the need for interdisciplinary treatment in the ICU setting, even if patients do not primarily present with myositis-associated medical issues.
Patient characteristics
| Number of included patients | 23 | |
|---|---|---|
| Female patients n (% ) | 15 (65) | |
| Age in years, mean (min-max ) | 58 (19-83) | |
| Disease duration in years, mean (min-max ) | 13 (0-38) | |
| Duration of ICU stay in days, mean (min-max ) | 32 (1-503) | |
| Admission from n (% ) | Emergency room | 6 (26) |
| General ward | 11 (48) | |
| Other hospital | 6 (26) | |
| Discharge n (% ) | General ward | 14 (61) |
| Death | 5 (22) | |
| Rehabilitation | 2 (9) | |
| Other | 2 (9) | |
| Re-admission to ICU n (% ) | 5 (22) | |
| Immunosuppressive treatment at time of ICU admission n (% ) | Glucocorticoids | 20 (87) |
| Azathioprine | 5 (22) | |
| Intravenous immunoglobulins | 3 (13) | |
| Rituximab | 2 (9) | |
| Mycophenolate mofetil | 2 (9) | |
| Hydroxychloroquine | 2 (9) | |
| JAK-inhibition | 1 (4) | |
| Cyclophosphamide | 1 (4) | |
| Methotrexate | 1 (4) | |
| None | 2 (9) | |
| Infectious complication n (% ) | All infections | 11 (48) |
| Pulmonary infection | 11 (100) | |
| Viral infection (CMV, HSV, SARS-CoV2) | 2 (18) | |
| Bacterial infection | 6 (55) | |
| Fungal infection (PJP) | 1 (9) | |
| No pathogen detected | 4 (36) | |
| Abdominal infection | 3 (27) | |
| Catheter-associated infection | 2 (18) | |
| Urogenital infection | 1 (9) | |
| Gastrointestinal infection | 1 (9) |
Myositis patients in the intensive care unit (ICU). a) Reason of ICU admission. b) Myositis subtype of treated patients. c) Active organ involvement during ICU stay. d) Most common comorbidities of patients
REFERENCES: NIL.
Acknowledgements: K. Roedl and M. Krusche contributed equally and share last authorship.
Disclosure of Interests: Marie-Therese Holzer: None declared, Johann Herzig: None declared, Simon Melderis: None declared, Dominic Wichmann: None declared, Paymon Ahmadi: None declared, Margherita Giannini: None declared, Ina Kötter Abbvie, Janssen, Lilly, Medac, Novartis and Sobi, Boehringer, GSK and Eusapharma, Stefan Kluge: None declared, Alain Meyer: None declared, Kevin Roedl: None declared, Martin Krusche: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (