fetching data ... 
Background: Gout is a common metabolic disease with an increasing annual incidence. However, current first-line treatment options remain limited. Inhibition of the pro-inflammatory cytokine interleukin (IL)-1β has demonstrated efficacy in reducing pain and inflammation in patients with gout [1]. Treatment with genakumab, an anti-IL-1β monoclonal antibody, has demonstrated superior sustained control of acute gout flares compared with control in the second-line setting [2], highlighting its potential as a novel first-line therapeutic option for patients with gout.
Objectives: To assess the efficacy and safety of genakumab vs etoricoxib for first-line treatment in patients with acute gout flare.
Methods: This phase 2, multicenter, randomized, open-label, active controlled study (NCT05936268) was conducted across 37 centers in China. Eligible patients were adults aged 18–75 years with gout who had experienced at least two gout flares in the 12 months prior to screening. Patients were randomized 1:1 to receive either a single subcutaneous injection of genakumab 200 mg or etoricoxib 120 mg orally once daily until remission or intolerance for ≤8 days. In cases of acute gout flares following treatment, an additional single 200 mg genakumab injection could be administered. The treatment period was 12 weeks, with safety follow-up continuing for 12 weeks after the last dose. The primary efficacy endpoint was the change from baseline in target joint pain at 72 hours post-treatment, assessed using a 0–100 mm visual analogue scale (VAS). Non-inferiority was evaluated using a mixed model for repeated measures (MMRM) with a 10 mm upper 95% confidence interval (CI) threshold. If non-inferiority was established, superiority testing was performed with a 0 mm threshold. Secondary endpoints included: 1) change from baseline in VAS score at 6, 24, and 48 hours, and 7 days post-treatment; 2) time to at least 50% reduction from baseline in VAS score; 3) proportion of patients with at least one relapse; and 4) time to relapse during treatment. Safety was evaluated through the monitoring of adverse events (AEs) and laboratory assessments. The immunogenicity of genakumab was also assessed.
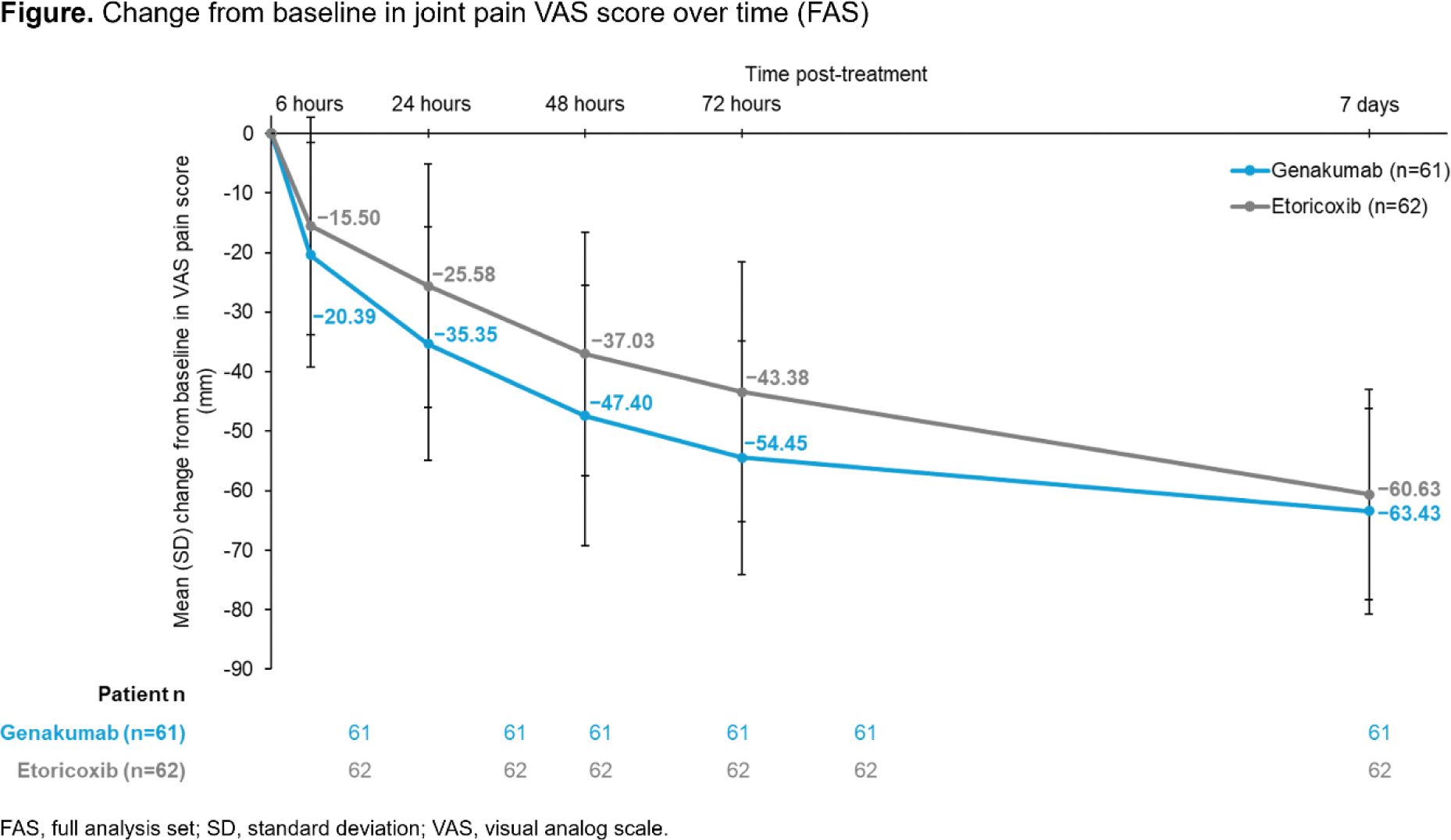
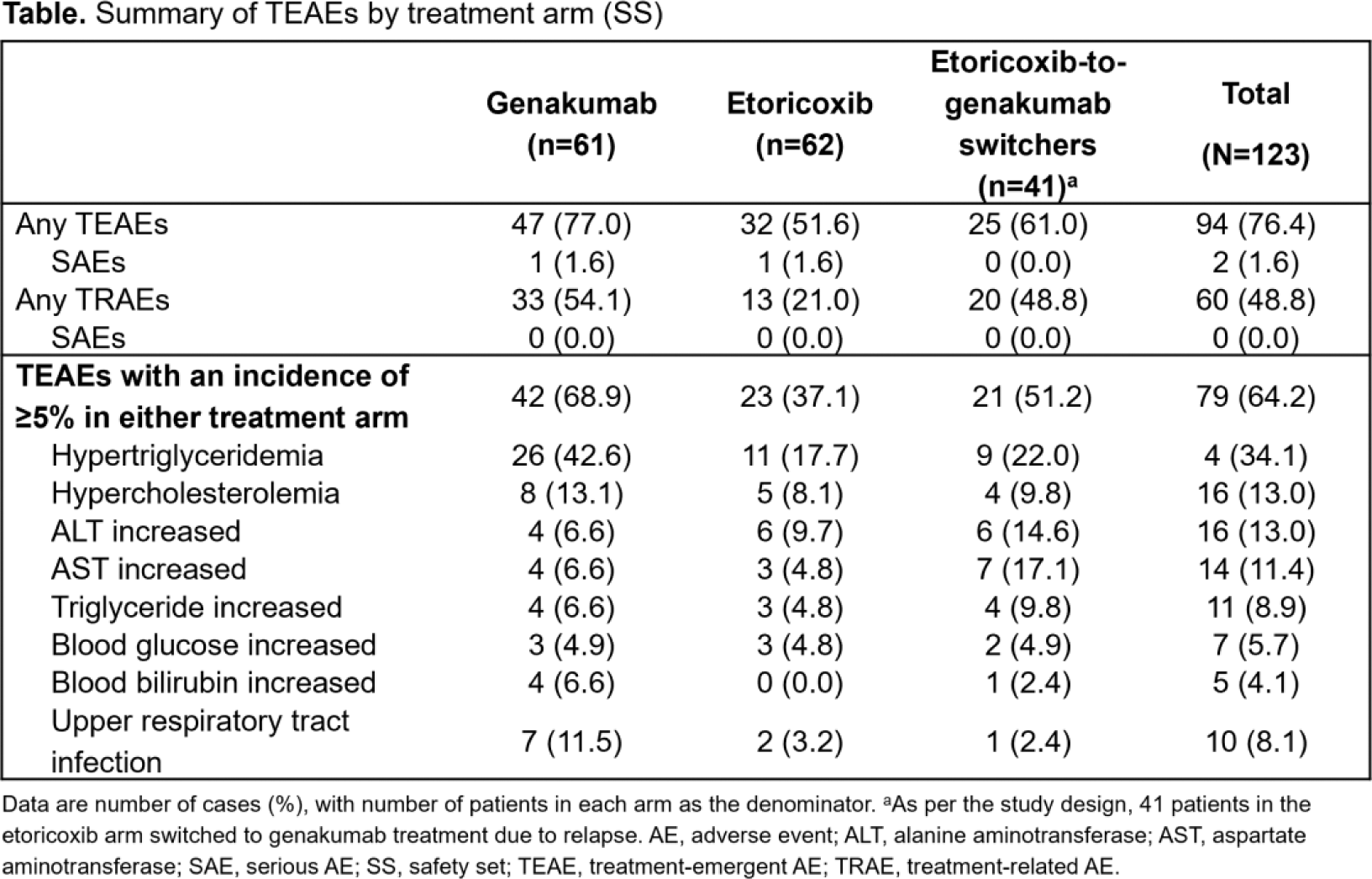
Results: Between July 19, 2023, and February 28, 2024, a total of 125 patients were randomized, of whom 123 received genakumab (n=61) or etoricoxib (n=62). Baseline demographics and disease characteristics were generally comparable between the genakumab and etoricoxib arms: 98.4% vs 100.0% were male; the mean (SD) age was 41.2 (11.0) vs 40.2 (11.7) years; mean BMI was 26.6 (4.1) vs 27.3 (3.3) kg/m2; and the median (Q1, Q3) duration of gout was 80.0 (43.8, 127.5) vs 80.2 (43.0, 123.2) months, respectively. At 72 hours post treatment, the least squares mean (LSM) change from baseline in VAS score was −54.37 mm in the genakumab arm, vs −43.46 mm in the etoricoxib arm; the LSM difference was −10.91 (95% CI: −18.11, −3.72) mm, demonstrating non-inferiority and superiority of genakumab over etoricoxib in reducing acute joint pain during gout flares. VAS scores decreased in both arms after treatment but were consistently lower in the genakumab arm at all timepoints (Figure 1). The median time to at least 50% pain reduction was 2.0 (95% CI: 2.0, 3.0) vs 4.0 (95% CI: 3.0, 4.0) days for genakumab and etoricoxib, respectively (HR: 1.7, 95% CI: 1.1, 2.4; p=0.0017), indicating a faster onset of pain relief with genakumab. Gout relapse was less frequent with genakumab; 6.6% (n=4) of patients experienced a flare within 12 weeks vs 66.1% (n=41) in the etoricoxib arm. The median time to first relapse was not reached in the genakumab arm, compared with 28.0 days (95% CI: 21.0, 52.0) in the etoricoxib arm (HR: 0.1, 95% CI: 0.0, 0.2; p<0.0001). Overall, 76.4% (n=94) of patients experienced at least one treatment-emergent AE (TEAE); with an incidence of 77.0% (n=47) in the genakumab arm and 51.6% (n=32) in the etoricoxib arm (Table 1). The lower incidence of TEAEs in the etoricoxib arm may be explained by shorter drug exposure among the 41 patients who switched to genakumab treatment, leading to incomplete 12-week safety data for this patient subset. The most common TEAE in both arms was hypertriglyceridemia (42.6% [n=26] vs 17.7% [n=11] in the genakumab and etoricoxib arms, respectively). No TEAEs led to study discontinuation, and no treatment-related Serious AEs or deaths were reported. Additionally, 12.7% (n=13) of patients tested positive for anti-drug antibodies (ADAs); 7.8% (n=8) became ADA positive after treatment.
Conclusion: Compared with daily oral etoricoxib, a single 200 mg subcutaneous injection of genakumab provides faster, more sustained relief of joint pain over 12 weeks, reduces recurrence risk, and is well tolerated as a first-line treatment for gout flares.
REFERENCES: [1] Schlesinger N, et al. Arthritis Res Ther. 2023;25(1):128.
[2] Xue Y, et al. Arthritis Rheumatol. 2024;76(Suppl 9) [Abstract 0278].
Acknowledgements: This study was sponsored by Changchun GeneScience Pharmaceutical Co., Ltd. Medical writing support was provided by Daisy Toplass, MSc (Rude Health Consulting Ltd), and was sponsored by Changchun GeneScience Pharmaceutical Co., Ltd.
Disclosure of Interests: Hejian Zou: None declared, Yu Xue: None declared, Li Mao: None declared, Long Qian: None declared, Hongtao Guo: None declared, Jiankang Hu: None declared, Fenghong Yuan: None declared, Rongbin Li: None declared, Xinwang Duan: None declared, JING YU: None declared, Wei Gou: None declared, Lei Yang: None declared, Hua Wei: None declared, Rongping Li: None declared, JIANGTAO LI: None declared, Jing Yang: None declared, li Qin: None declared, Anbin Huang: None declared, Ning Zhang: None declared, Yanlin Li: None declared, Zhichun Liu: None declared, li shujie: None declared, Zhenchun Zhang: None declared, Shengyun Liu: None declared, Jie Wu: None declared, Lihua Duan: None declared, Hua Shang: None declared, Ling Lei: None declared, Jingyang Li: None declared, Xuebin Wang: None declared, Zili Fu: None declared, Zhengfu Du: None declared, Lin Chen: None declared, Xiaofei Shi: None declared, Juan Li: None declared, Jianzhao Cheng: None declared, Qingchu Li: None declared, Zhanqing Gu: None declared, Jiashun Zeng: None declared, Qian Xu Employee of Changchun GeneScience Pharmaceutical Co., Ltd., Tianhong Luo Employee of Changchun GeneScience Pharmaceutical Co., Ltd.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (