fetching data ... 
Background: Neuropsychiatric (NP) involvement is a potentially severe complication of systemic lupus erythematosus (SLE), significantly increasing the disease burden. It contributes to substantial organ damage, disability, and higher mortality rates compared to SLE patients without neuropsychiatric manifestations. Among the factors implicated in the pathogenesis of neuropsychiatric lupus erythematosus (NPLE), anti-ribosomal Ribonucleoprotein (anti-rRNP) antibodies are thought to play a pivotal role. Further analysis of the impact of anti-rRNP positivity on NPLE characteristics is essential.
Objectives: This study aims to conduct a comparative analysis of patients with and without anti-rRNP positivity to provide deeper insights into the phenotypic variations of NPLE.
Methods: Retrospective collection of clinical data from NPLE patients hospitalized at Peking Union Medical College Hospital from 2019 to 2024. All the patients met the 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. NP involvements were diagnosed according to ACR nomenclature and case definitions for NPSLE in 1999. Patients with secondary causes of neuropsychiatric manifestations, such as central nervous system (CNS) infections or non-SLE-related CNS diseases, were excluded from the study. Clinical, demographic and serological features were collected. For patients undergoing lumbar puncture, cerebrospinal fluid (CSF) examination results will also be collected. Additionally, patients were stratified based on their anti-rRNP antibody status (positive or negative) to facilitate a comparative analysis of clinical and serological features. Statistical analyses were performed to evaluate group differences, with significance defined as P<0.05.
Results: A total of 425 NPLE patients were included in the study, with a median age of 33 years (IQR 26–42), of whom 87% were female. CNS involvement was predominant (93.6%), with 635 instances reported. The most common CNS manifestations included seizure disorders (153 cases), acute confusional states (152), cerebrovascular disease (87), and cognitive dysfunction (47). Peripheral nervous system (PNS) involvement was less frequent (6.4%) (Figure 1). For other system manifestations, mucocutaneous involvement was prevalent, including acute cutaneous lupus erythematosus/subacute cutaneous lupus erythematosus(ACLE/SCLE) (205 patients), non-scarring alopecia (123), and mucosal ulcers (166). Hematological manifestations were also common, with leukopenia observed in 226 patients (53%), thrombocytopenia in 190 (45%), and hemolytic anemia in 81 (19%). Lupus nephritis was diagnosed in 246 patients (58%), while musculoskeletal involvement, primarily arthritis, was noted in 166 patients (39%). Autoantibody profiles revealed high positivity rates for anti-dsDNA (278, 65%) and anti-SSA (253, 60%), alongside reduced complement levels (median C3: 0.62 g/L; C4: 0.10 g/L). The median SLEDAI score was 14 (IQR 9–21), indicating significant disease activity. Among 323 patients who underwent lumbar puncture, the median cerebrospinal fluid (CSF) pressure was 150 mmH 2 O (IQR 120–195), with increased intracranial pressure (ICP) reported in 100 cases (31%). The median CSF white blood cell (WBC) count was 2×10⁶/L (IQR 0–3), and the median CSF protein level was 0.37 g/L (IQR 0.28–0.56), with elevated protein levels observed in 111 patients (34%). Patients with anti-rRNP positivity (n=140) exhibited distinct clinical and laboratory features compared to anti-rRNP negative patients (n=285) (Table 1). Mucocutaneous involvement, including ACLE/SCLE (56.4% vs. 44.2%, P=0.02), CCLE (12.9% vs. 6.7%, P=0.03), and non-scarring alopecia (39.3% vs. 23.9%, P=0.001), was more common in the positive group, as were leukopenia (64.3% vs. 47.7%, P=0.001), lupus nephritis (60.7% vs. 34.4%, P<0.001), and musculoskeletal involvement (28.6% vs. 19.6%, P=0.04). Anti-rRNP positive patients had higher positivity rates for anti-dsDNA (72.9% vs. 62.1%, P=0.003), anti-Sm (42.9% vs. 29.8%, P=0.008), anti-RNP (52.9% vs. 35.4%, P=0.001), and anti-SSA (69.3% vs. 54.7%, P=0.004), alongside lower C3 (0.54 vs. 0.67 g/L, P=0.001) and C4 levels (0.09 vs. 0.10 g/L, P=0.02). CSF analysis revealed higher protein levels (median: 0.43 vs. 0.36 g/L, P=0.045) and more frequent elevated protein (35.7% vs. 21.4%, P=0.002) in the positive group, with lower glucose levels (3.1 vs. 3.3 mmol/L, P=0.031).
Conclusion: Anti-rRNP positive patients exhibited distinct clinical, serological, and cerebrospinal fluid characteristics, may reflecting unique phenotypic features within NPLE.
Distribution of neuropsychiatric events attributed to SLE
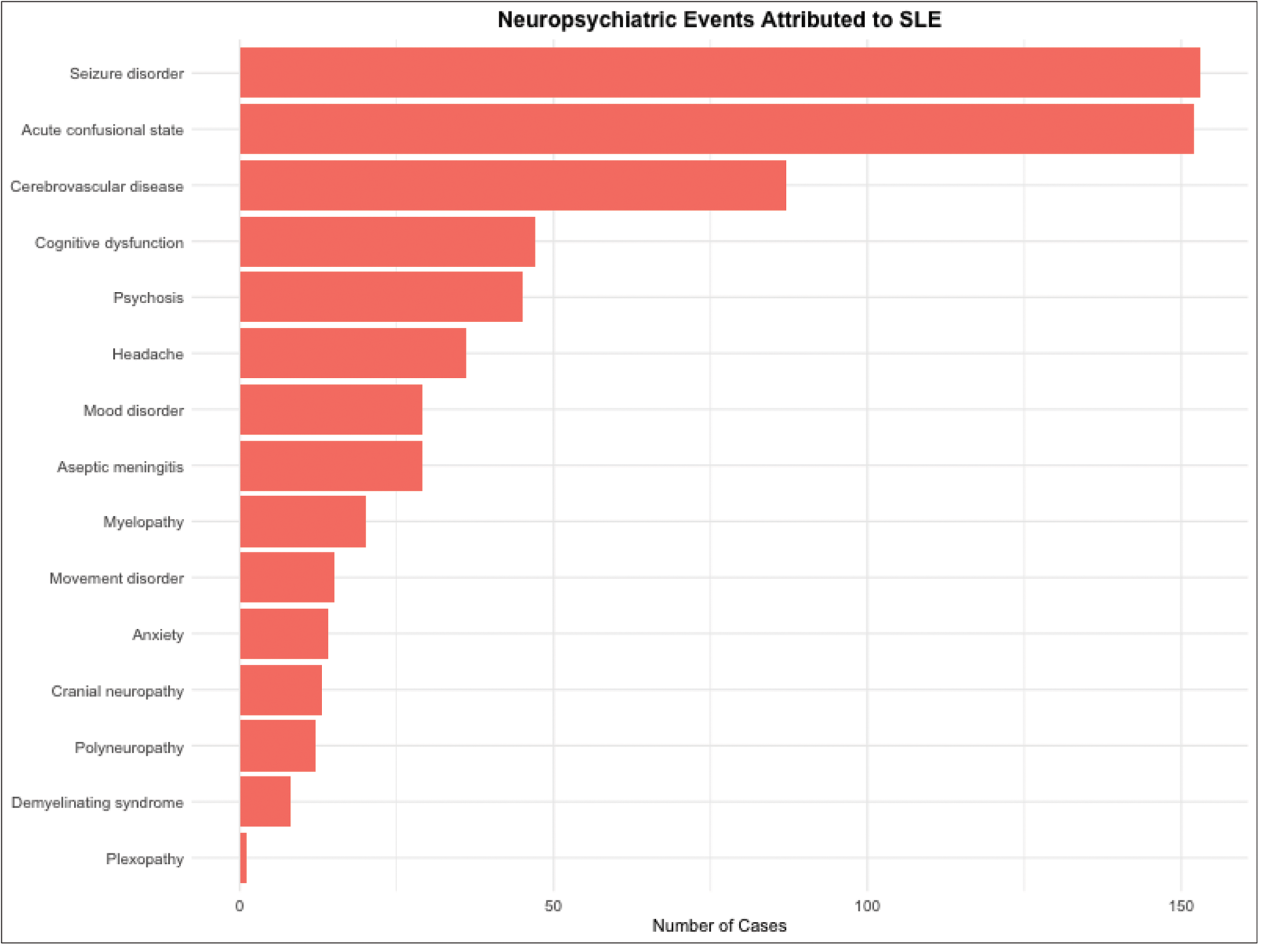
Table 1. Comparison of baseline demographics, clinical, and serological features between anti-rRNP positive and negative NPLE patients
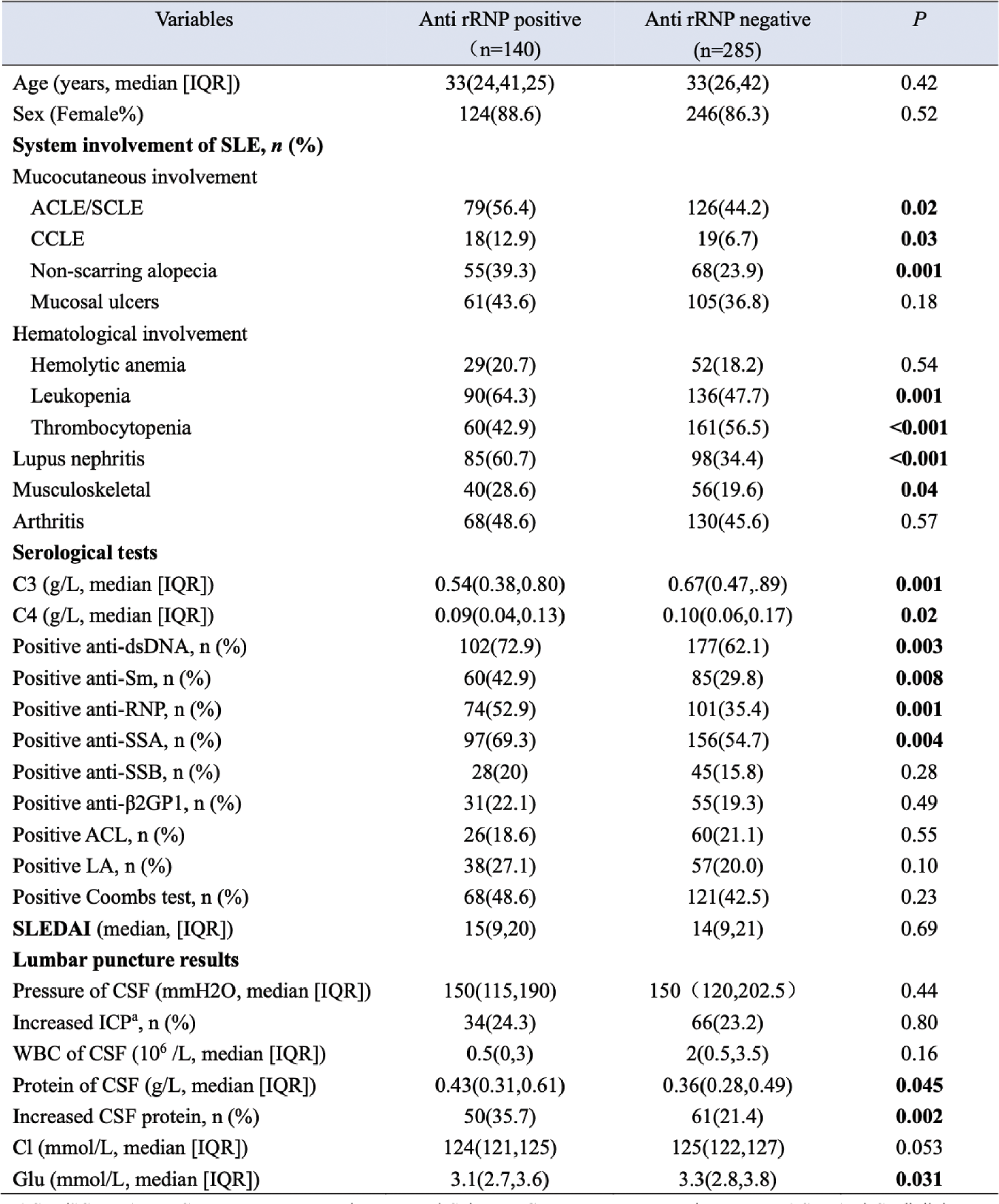
ACLE/SCLE, Acute Cutaneous Lupus Erythematosus/ Subacute Cutaneous Lupus Erythematosus; ACL, Anti-Cardiolipin Antibody; CCLE, Chronic Cutaneous Lupus Erythematosus; CSF, Cerebrospinal Fluid; ICP, Intracranial Pressure; LA, Lupus Anticoagulant; NPLE, neuropsychiatric lupus erythematosus; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index; anti-rRNP antibody, Anti-Ribosomal Ribonucleoprotein Antibody.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (