fetching data ... 
Background: Bimekizumab (BKZ) is a monoclonal IgG1 antibody that selectively inhibits interleukin (IL)-17F in addition to IL-17A. Sustained and consistent efficacy and safety have been demonstrated up to 2 years in patients with active psoriatic arthritis (PsA) who were biologic disease-modifying antirheumatic drug (bDMARD)-naïve or had prior inadequate response or intolerance to tumour necrosis factor inhibitors [1].
Objectives: To assess long-term efficacy and safety of BKZ treatment up to 3 years in patients with active PsA who were bDMARD-naïve.
Methods: In BE OPTIMAL (NCT03895203), patients with PsA who were bDMARD-naïve were randomised 3:2:1 to subcutaneous BKZ 160 mg every 4 weeks (Q4W), placebo (PBO) or a reference arm (adalimumab [ADA] 40 mg Q2W). PBO patients switched to BKZ at Week 16 (PBO/BKZ); ADA patients switched to BKZ at Week 52 with no washout between treatments (ADA/BKZ). Patients completing Week 52 were eligible for entry into BE VITAL (open-label extension [OLE]; NCT04009499). Efficacy and safety data reported here are from the BE OPTIMAL/BE VITAL study. Efficacy outcomes are reported to Week 160 for patients in the BKZ Total group (PBO/BKZ patients and BKZ-randomised patients; providing a total duration of therapy of 144 or 160 weeks, respectively). Missing data were imputed using modified non-responder (mNRI; binary), multiple (MI; continuous) or worst-category (WCI; categorical) imputation. mNRI considered all visits following discontinuation due to adverse events or lack of efficacy as non-response; all other missing data were imputed with MI and the response derived from the imputed values. Safety data are reported to Week 156 for all randomised patients who received at least one dose of BKZ (BKZ-treated patients). All treatment-emergent adverse events (TEAEs) were classified using the Medical Dictionary for Regulatory Activities v19.0.
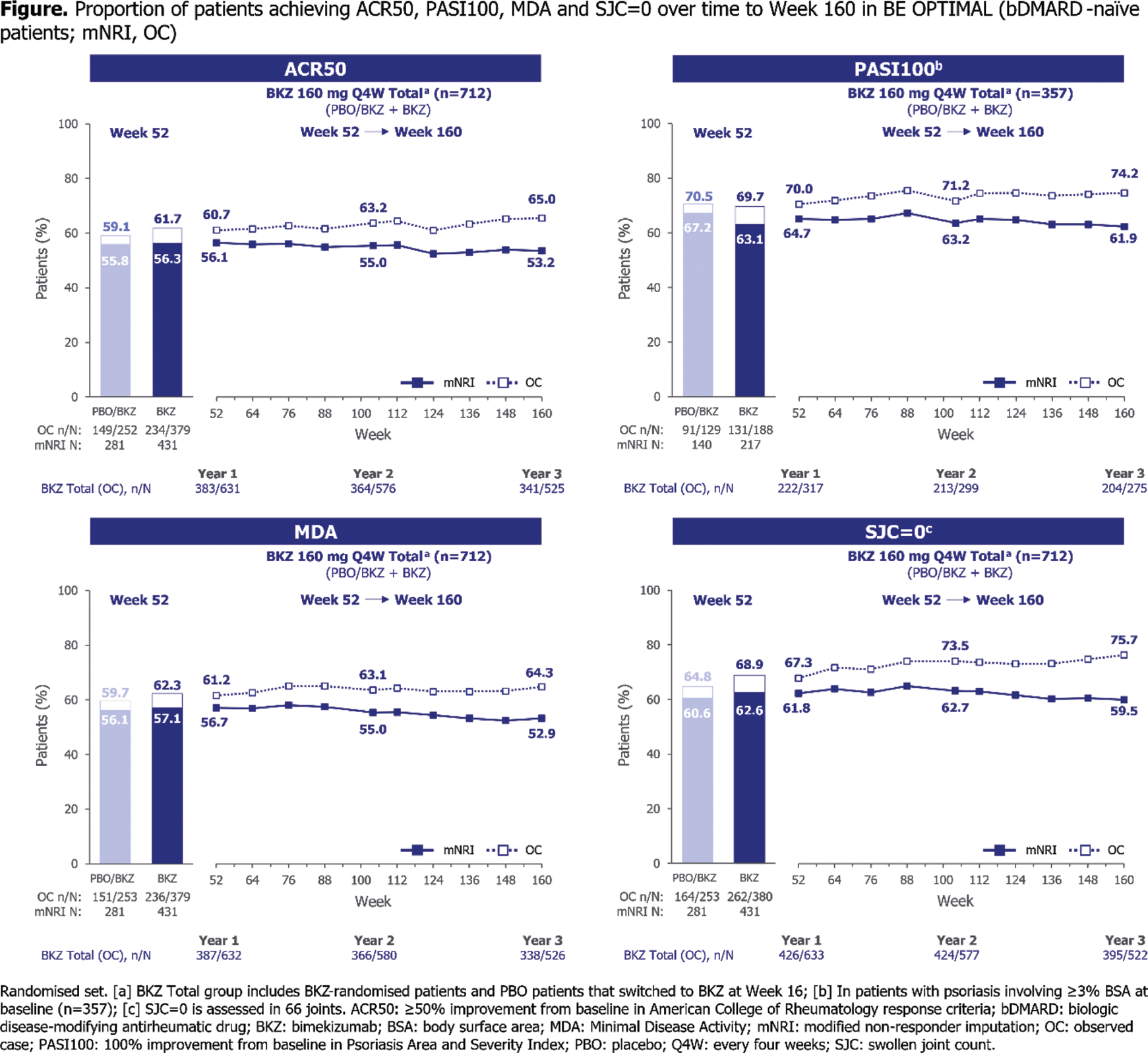
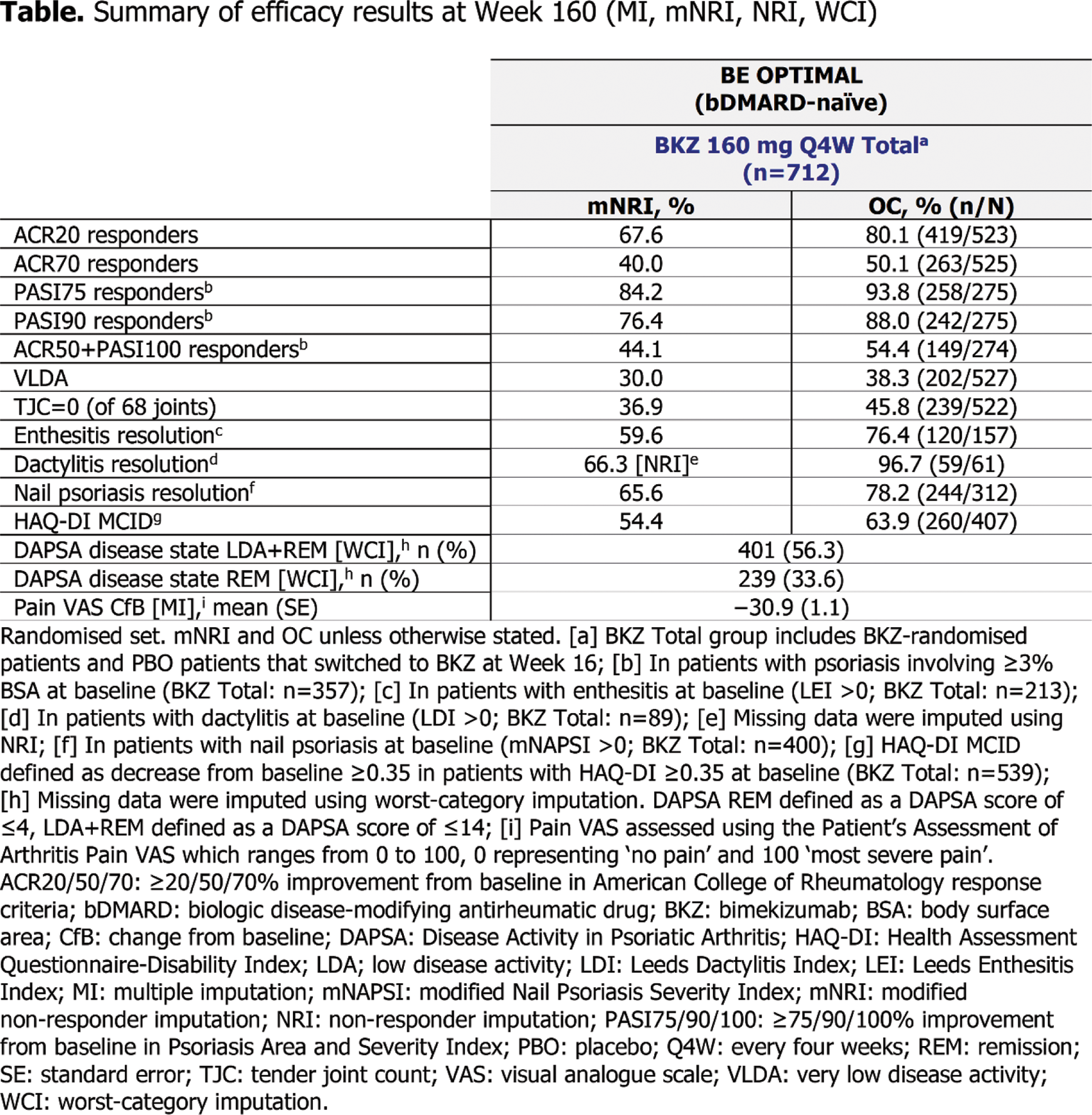
Results: Overall, 654/852 (76.8%) patients completed Week 160 (546/712 [76.7%] patients in the BKZ Total group). Across all efficacy outcomes, patients in the BKZ Total group demonstrated sustained clinical responses through 3 years. The proportion of patients achieving ≥50% improvement from baseline in American College of Rheumatology response criteria (ACR50) was sustained from 56.1% at Week 52 to 53.2% at Week 160 (Figure 1). In patients with baseline psoriasis (≥3% body surface area), complete skin clearance (Psoriasis Area and Severity Index [PASI]100) response was sustained from 64.7% at Week 52 to 61.9% at Week 160 (Figure 1). The proportion of patients reaching minimal disease activity (MDA) was sustained from 56.7% at Week 52 to 52.9% at Week 160 (Figure 1). The proportion of patients achieving resolution of swollen joint count (SJC=0), a clinical measure of inflammation, was sustained from 61.8% at Week 52 to 59.5% at Week 160 (Figure 1). Similar sustained responses from Week 52 were observed at Week 160 for additional efficacy outcomes (Table 1). ADA/BKZ patients demonstrated similar sustained clinical responses across all efficacy outcomes through 3 years. Over 3 years, the incidence rate (exposure-adjusted incidence rate [EAIR]/100 patient years [PY]) for BKZ-treated patients reporting ≥1 TEAE was 164.2 (95% confidence interval [CI]: 152.7, 176.3); incidence of serious TEAEs was 6.5 (5.4, 7.8). The three most frequent TEAEs by preferred term were SARS-CoV-2 (COVID-19) infection (EAIR/100 PY: 12.7 [95% CI: 11.1, 14.5]), nasopharyngitis (7.8 [6.6, 9.3]) and upper respiratory tract infection (6.1 [5.0, 7.4]). The number of reported cases were low for adjudicated major adverse cardiovascular events (9; EAIR/100 PY: 0.5 [95% CI: 0.2, 0.9]), serious infections (28; 1.4 [0.9, 2.0]), adjudicated definite or probable inflammatory bowel disease (7; 0.4 [0.1, 0.7]), malignancies (excluding non-melanoma skin cancer; 9; 0.5 [0.2, 0.9]) and adjudicated suicidal ideation and behaviour (2; 0.1 [0.0, 0.4]). Hepatic events occurred in 105 patients (EAIR/100 PY: 5.7 [95% CI: 4.7, 6.9]). Three deaths were reported up to 3 years, all deemed unrelated to study treatment by the investigator. Up to 3 years, the incidence rate of fungal infections was 9.2 (95% CI: 7.9, 10.8), none were systemic and the majority identified as Candida infections (EAIR/100 PY: 5.7 [95% CI: 4.7, 6.9]); most Candida infections were oral candidiasis (4.3 [3.4, 5.4]). One case of a serious Candida infection (oropharyngeal candidiasis) was reported up to 3 years. The number of patients discontinuing therapy due to Candida infections was low (7; EAIR/100 PY: 0.4 [95% CI: 0.1, 0.7]).
Conclusion: Efficacy results from the final full year of BE OPTIMAL and its OLE demonstrated that BKZ treatment results in sustained clinical efficacy up to 3 years in patients with active PsA who were bDMARD-naïve. BKZ was well tolerated with a favourable safety profile and no new safety signals were observed [1, 2].
REFERENCES: [1] Mease PJ. Rheumatol Ther 2024;11:1363–82; 2. Ritchlin CT. Ann Rheum Dis 2023;82:1404–14.
Acknowledgements: Funded by UCB. Medical writing support provided by Costello Medical and funded by UCB.
Disclosure of Interests: Laure Gossec Consulting fees from AbbVie, Amgen, BMS, Celltrion, Janssen, Lilly, MSD, Novartis, Pfizer and UCB, Grants or contracts from AbbVie, Biogen, Lilly, Novartis and UCB, Laura C. Coates Speaking fees from AbbVie, Amgen, Biogen, Celgene, Eli Lilly, Galapagos, Gilead, GSK, Janssen, medac, Novartis, Pfizer and UCB, Consultant for AbbVie, Amgen, BMS, Boehringer Ingelheim, Celgene, Domain, Eli Lilly, Galapagos, Gilead, Janssen, Moonlake Immunotherapeutics, Novartis, Pfizer and UCB, Grant/research support from AbbVie, Amgen, Celgene, Eli Lilly, Gilead, Janssen, Novartis, Pfizer and UCB, Iain B. McInnes Consulting fees and honoraria from AbbVie, AstraZeneca, BMS, Boehringer Ingelheim, Cabaletta, Causeway Therapeutics, Celgene, Eli Lilly and Company, Evelo, Janssen, MoonLake Immunotherapeutics, Novartis and UCB, Research support from BMS, Boehringer Ingelheim, Celgene, Janssen, Novartis and UCB, Philip J. Mease Speakers bureau fees from AbbVie, Amgen, Eli Lilly and Company, Janssen, Novartis, Pfizer and UCB, Consulting fees from AbbVie, Acelyrin, Amgen, BMS, Cullinan, Eli Lilly and Company, GSK, Inmagene, Janssen, Moonlake Pharma, Novartis, Pfizer, Takeda, UCB and Ventyx, Research grants from AbbVie, Acelyrin, Amgen, BMS, Eli Lilly and Company, Janssen, Novartis, Pfizer, Sana and UCB, Christopher T. Ritchlin Consultant for AbbVie, Amgen, BMS, Eli Lilly, Janssen, MoonLake, Novartis, Pfizer, Solarea and UCB, Research for AbbVie, Yoshiya Tanaka Speaker fees and/or honoraria from AbbVie, Asahi-kasei, Astellas, AstraZeneca, Boehringer Ingelheim, Chugai, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, GSK, Pfizer, Taisho and UCB, Grants from Boehringer Ingelheim, Chugai and Taisho, Akihiko Asahina Research grants and/or honoraria from AbbVie, Amgen, BMS, Boehringer Ingelheim, Eisai, Eli Lilly, Janssen, Kyowa Kirin, LEO Pharma, Maruho, Mitsubishi Tanabe Pharma, Novartis, Pfizer, Sun Pharma, Taiho Pharma, Torii Pharmaceutical Co. and UCB, Barbara Ink Shareholder of AbbVie, GSK and UCB, Employee of UCB, Rajan Bajracharya Shareholder of UCB, Employee of UCB, Jason Coarse Shareholder of UCB, Employee of UCB, Joseph F. Merola Consultant for AbbVie, Amgen, AstraZeneca, Biogen, BMS, Boehringer Ingelheim, Dermavant, Eli Lilly and Company, Incyte, Janssen, LEO Pharma, MoonLake Immunotherapeutics, Novartis, Pfizer, Sanofi-Regeneron, Sun Pharma and UCB.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (