fetching data ... 
Background: Recurrent monoarthritis (RM) is a common challenge in rheumatology, often linked to inflammatory conditions. While treatment typically includes NSAIDs, corticosteroids, DMARDs, and biologics, resistant cases may require frequent interventions, posing risks such as infection, side effects, and mechanical complications. Local measures like intra-articular aspiration (IAA) and corticosteroid injections offer temporary relief but are limited by recurrence and procedural intervals. Surgical and medical synovectomy, once considered for refractory cases, have been largely abandoned due to complications and low success rate. Ablation, a minimally invasive technique, has emerged as a novel option for RM. Microwave ablation (MWA), targeting hypertrophied synovial tissue, has shown promise in controlling RM attacks. Our initial studies demonstrated its safety and efficacy, paving the way for broader applications in resistant monoarthritis.
Objectives: We aimed to assess the long term results of MWA technique in a larger cohort as an adjunctive therapy in patients with different rheumatic diseases suffering from recurrent monoarthritis resistant to medical treatment with confirmed synovial hypertrophy in terms of safety and effectivity.
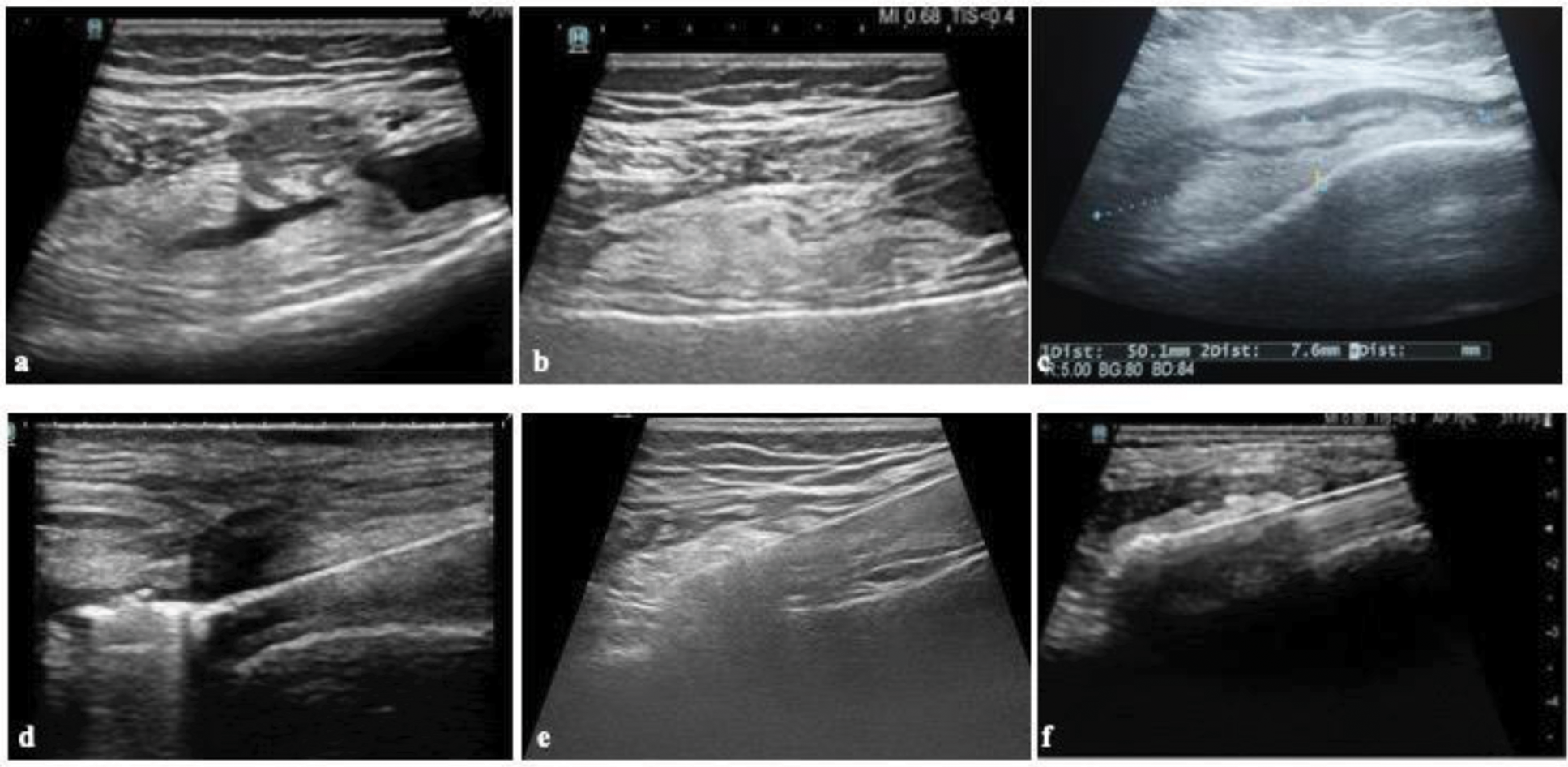
Methods: Patients with inflammatory diseases leading to recurrent monoarthritis (RM) were included. Procedures were performed by two interventional radiologists: one for the majority of cases and another for the last eight patients to eliminate operator dependency and demonstrate reproducibility. After surgical asepsis and local anesthesia, antimicrobial prophylaxis with ampicillin/sulbactam and sedation with midazolam and fentanyl were applied. Synovial hypertrophy was assessed using ultrasound (USG), and significant fluid, if present, was aspirated. A monopolar MWA probe with internal cooling was placed via a 2 mm skin incision under USG guidance. Ablation was performed using 15–20W energy with the moving-shot technique until microbubbles, indicating necrosis, were observed (Figure 1). For larger hypertrophies, multiple ablation zones were treated sequentially. Energy and ablation duration were recorded.
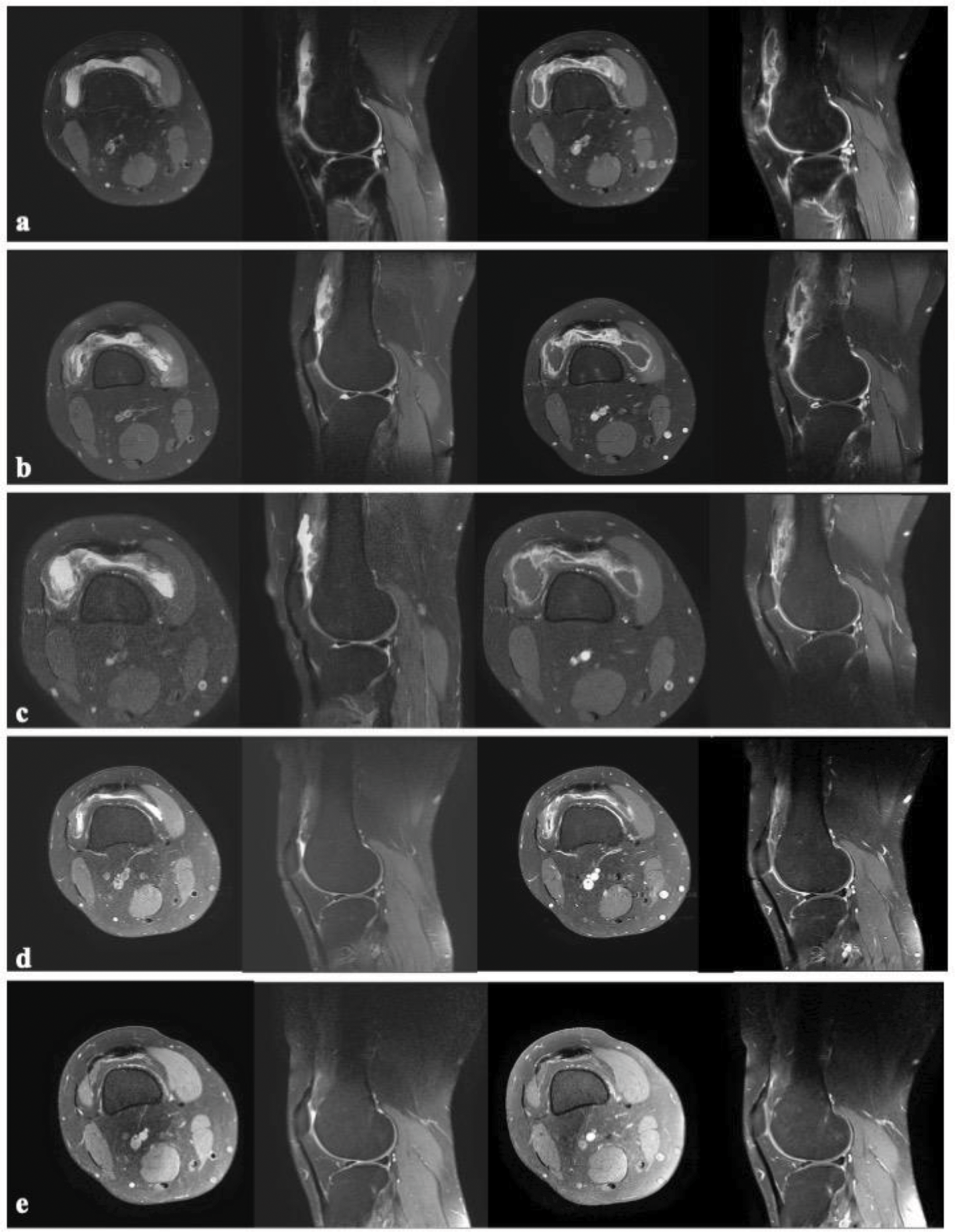
Results: We applied MWA to a total of 43 knee joints in 37 patients (18 female and 19 male) aged between 22 and 71 years. The median number of IAAn the six months prior to MWA was 5 (0–15). Three patients had previously undergone surgical synovectomy. In three knees of two patients, the number of IAAs in the last six months was 0; these patients had persistent synovial effusion and abundant synovial hypertrophy but declined IAA. A second MWA session was required in five patients, and one patient underwent a third. The median follow-up period was 15 months (5–25). The overall number of IAAs in the six months before MWA was 207 across a 258 months (0.81 per month). This decreased significantly to 21 IAAs over 624 cumulative months post-MWA (0.03 per month; p<0.001). Short-term, low-dose corticosteroid therapy was administered in 14 patients (16 knees). Challenges during follow-up that necessitated additional interventions included mechanical injuries, patient compliance issues, and infections, including COVID-19, which resulted in minor arthritis flares or elevated acute-phase reactants. Additional interventions included physical therapy or aspiration of Baker’s cysts, as well as injections to the Achilles tendon in seven patients. Following successful completion of six months post-procedure, corticosteroid reduction or cessation was achieved in 16 patients. Functional disability and pain scores showed significant improvement, with the median score decreasing from 9 to 1 (p < 0.0001 for both). No complications were observed during the procedure or follow-up. While both synovial hypertrophy and effusion persisted to varying degrees at the 1st and 3rd months on USG and MRI, IAA was deferred unless symptoms developed. Significant regression in synovial hypertrophy was demonstrated on MRI at the 6th month (Figure 2). A discordance between clinical improvement and radiological findings was observed in a small subset of the cohort.
Conclusion: MWA proved to be a safe and effective minimally invasive technique for managing RM with synovial hypertrophy, showing no complications. Over two years, the outcomes consistently aligned with initial findings, demonstrating significant reductions in the frequency of RM attacks and need for IAA, with additional substantial improvements in functional disability and pain scores. While persistent synovial fluid and hypertrophy were occasionally observed in the early months, significant regression of synovial hypertrophy was evident by the sixth month on MRI, correlating with sustained clinical improvements. For patients resistant to medical management, MWA offers a promising alternative to surgical interventions, providing effective control of symptoms and enhancing quality of life in the long term.
REFERENCES: NIL.
Microwave ablation technique showing the synovial hypertrophy tissue (a-b), measurement of the dimenisons (c), and, application of ablation probe and heating targeted synovial hypertrophy area (d, e, and f).
An example of a patient with pre-procedure (a), and post-procedure 1st (b), 3rd (c), 6th (d), and 12th (e) month MRI images indicating consistent improvement in MRI findings with time. In all rows, the order of images are positron density weighted (PDW) in the axial plane, PDW in the sagittal plane, T1-weighted contrast enhanced in the axial plane, and T1-weighted contrast enhanced in the sagittial plane, from left to right. Synovial hypertrophy and effusion did not show any significant change in the 1st and 3rd months after the procedure, whereas a significant regression was observed starting from the 6th month.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (