fetching data ... 
Background: Erosive hand osteoarthritis (ErHOA) is a severe form of hand osteoarthritis (HOA) associated with greater inflammation and disability. Previous studies exploring the relationship between osteoarthritis and the incidence of osteoporotic fractures have yielded inconsistent results, and data specifically on hand OA are limited.
Objectives: We aimed to investigate the association between ErHOA, bone loss, and the incidence of osteoporotic fractures.
Methods: We used data from the prospective QUALYOR study, which enrolled 1,575 postmenopausal women aged at least 50 years, followed prospectively for 14 years.
At baseline (the 6-year visit), HOA was assessed using hand radiographs and the AUSCAN questionnaire. Hand osteoarthritis status was defined as follows:
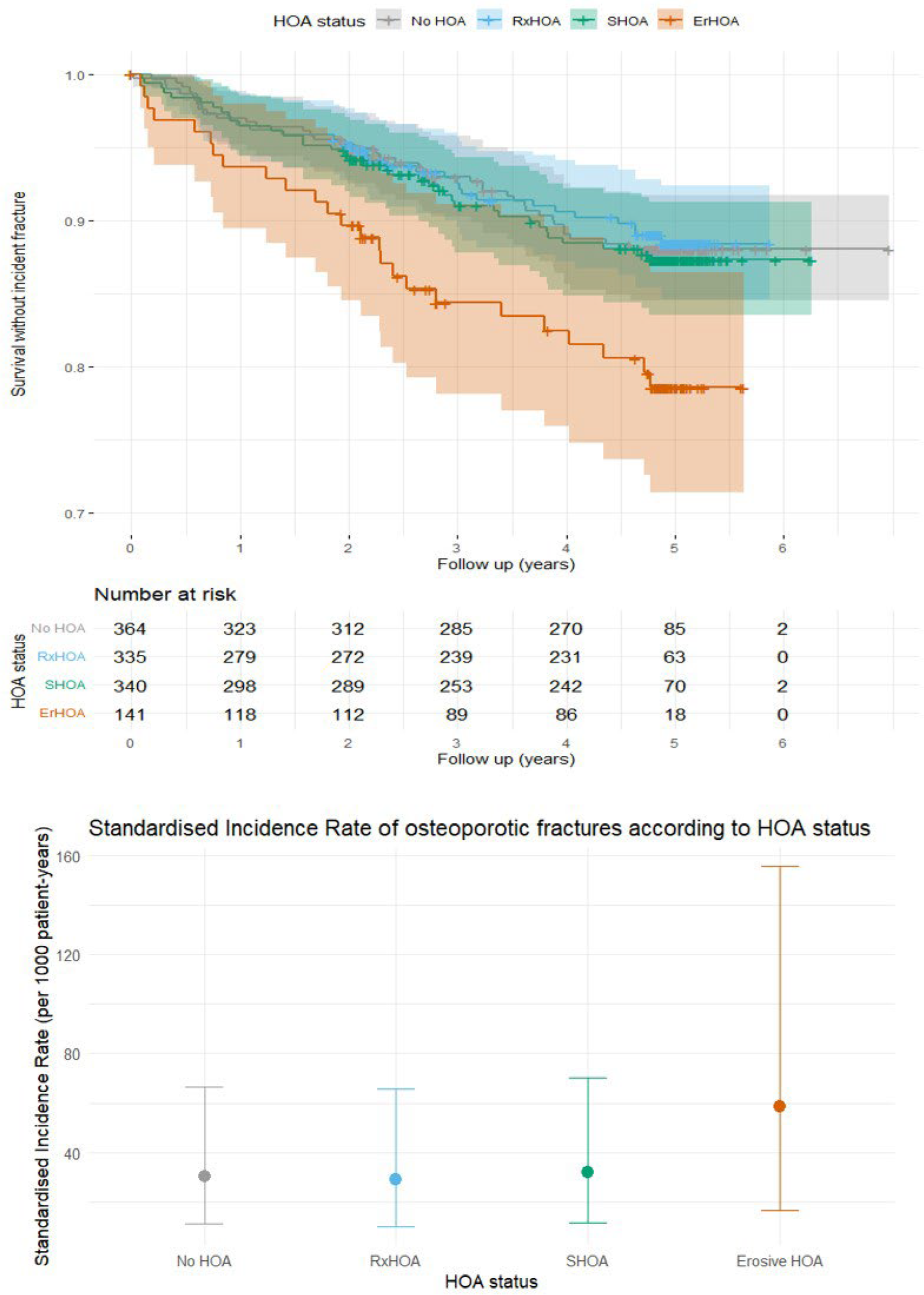
No HOA: no pain and no radiographic sign of HOA
Radiographic HOA (RxHOA): at least two joints graded KL ≥ 2 and no symptoms
Symptomatic HOA (SHOA): ACR criteria for HOA (no eroded joints)
Erosive HOA (ErHOA): SHOA with at least one eroded joint
Osteoporotic (OP) status was also evaluated at baseline and each follow-up visit by DXA (Bone Mineral Density [BMD] at the lumbar spine and hip), and incident OP fractures were medically ascertained. OP status was defined as follows:
No OP: all T-scores above −2.5 and no history of OP fracture
OP DXA: at least one T-score below −2.5 and no history of OP fracture
OP fracture: history of at least one OP fracture (regardless of T-scores)
Associations between baseline HOA status and incident OP fractures were analyzed using Cox proportional hazards models adjusted for age, fracture history, T-scores, obesity, and SPPB score (a surrogate marker of sarcopenia). Kaplan–Meier curves and standardized incidence rates (SIRs, Poisson regression) were obtained. Linear mixed-effects models adjusted for age and BMI assessed annual BMD changes according to HOA status. A mediation analysis evaluated the impact of ErHOA on incident fractures, with mediators selected among major fracture risk factors (age, T-scores, prevalent fracture at baseline, SPPB score).
Results: The analysis included 1,180 women (mean age 71.7 ± 6.4 years; mean follow-up 4.6 ± 0.9 years): 364 (30.8%) had no HOA, 335 (28.4%) RxHOA, 340 (28.8%) SHOA, and 141 (11.9%) ErHOA. Participants with ErHOA were significantly older, more obese, and more sarcopenic (lower SPPB scores) than controls. During follow-up, 131 participants (11.1%) experienced 166 incident OP fractures, with a mean time to event of 2.2 ± 1.42 years. Among them, 19.1% had ErHOA compared with 11.1% among those without incident fractures (p < 0.05). The age-standardized incidence rate of OP fractures was 58.5/1,000 patient-years (95% CI [16.6–155.7]) in ErHOA versus 30.2/1,000 patient-years (95% CI [10.9–66.6]) in participants without HOA or with non-erosive HOA. The hazard ratio (HR) for incident fracture in ErHOA compared with no HOA was 1.93 (95% CI [1.12–3.32], p < 0.05), whereas HRs were 1.10 (95% CI [0.69–1.77], n.s.) for SHOA and 0.95 (95% CI [0.59–1.57], n.s.) for RxHOA. Maxime.auroux. Additional stratification by prevalent fracture history at baseline (a major risk factor for subsequent OP fractures) again showed the highest fracture incidence rates in ErHOA patients.This increased fracture risk was not mediated by greater bone loss over time. Mediation analysis supported a predominant direct effect of ErHOA on fracture risk, outweighing all other mediators (direct effect = 0.379, p = 0.016).
Conclusions: Erosive HOA is a strong predictor of incident osteoporotic fractures in postmenopausal women, independently of classical fracture risk factors. These findings suggest that ErHOA represents a distinct endotype of HOA (since the association was not significant for other HOA phenotypes), and the mechanisms underlying this association warrant further integrated investigation.
Kaplan Meier curves and Standardised Incident rates of osteoporotic fractures according to hand osteoarthritis status
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.