fetching data ... 
Background: Deep B-cell depletion using T-cell engagers (TCEs) is an emerging therapeutic strategy in autoimmune diseases. We and others have previously reported the first successful treatments of various autoimmune diseases with the CD3×CD19 T-cell engager blinatumomab [1–3]. However, optimal dosing strategies and long-term benefits of blinatumomab in autoimmune diseases are poorly understood.
Objectives: While high-dose TCE regimens aim for maximal B-cell depletion, lower-dose protocols may optimize for safety benefits. Here, we present data on safety and clinical efficacy of low-dose blinatumomab in patients with active multidrug-resistant RA (MDR-RA).
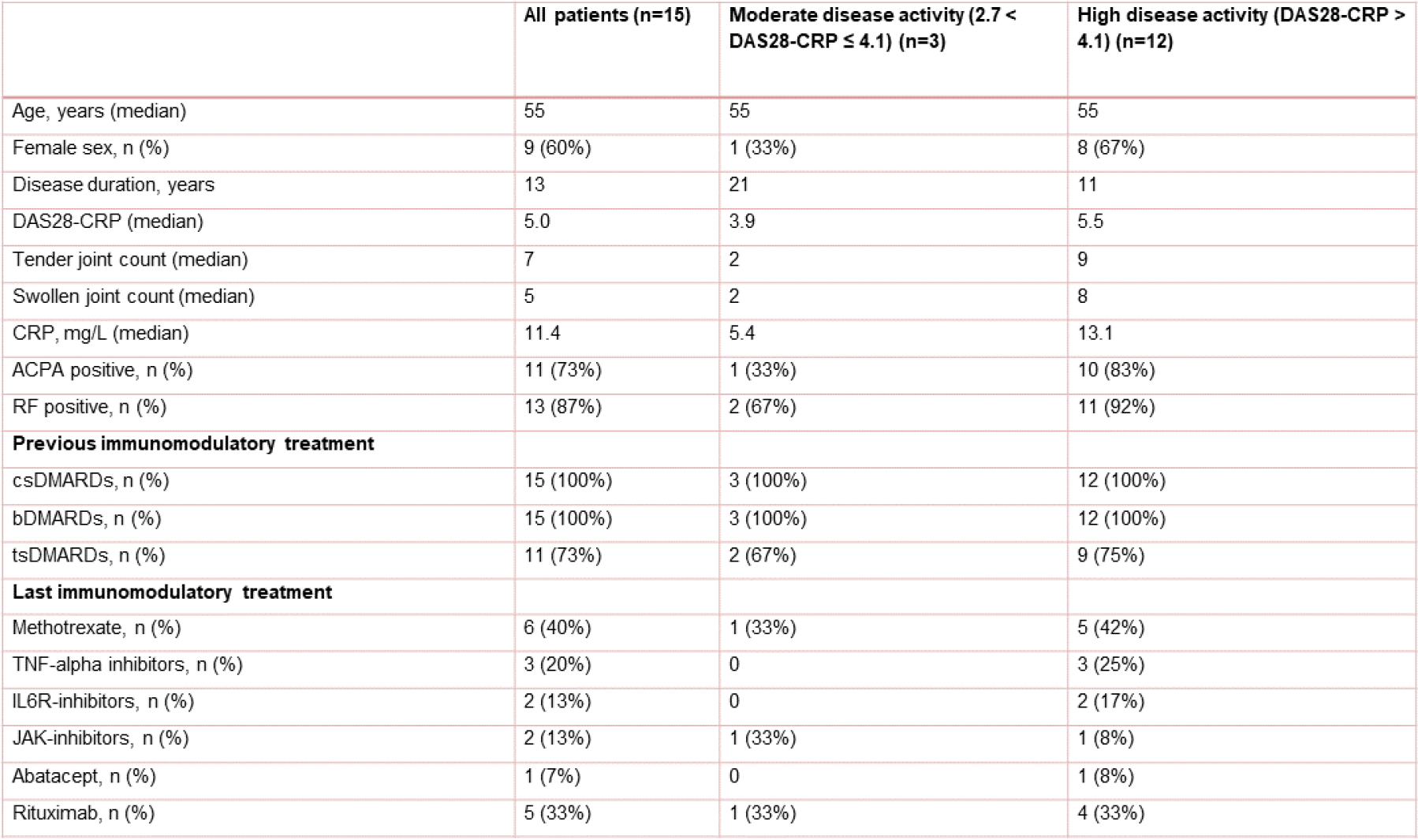
Methods: Blinatumomab was administered in an inpatient setting in fifteen patients with MDR-RA (Table 1). Patients received at least two cycles of blinatumomab, with each cycle administered as a continuous 96-hour infusion at 9 µg/day. Premedication consisted of 16 mg dexamethasone. The second cycle was initiated after a one-week treatment-free interval. The dose was increased to 28 µg/day in five patients in cycle 2 (patients #10, #12, #13, #14, #15), in one patient in cycle 3 (#9). Four patients received a third cycle of blinatumomab (#1, #4, #9, #12). We monitored safety (cytokine release syndrome, CRS; immune effector cell-related neurotoxicity syndrome, ICANS), clinical scores, and tissue inflammation via ultrasound and fibroblast activation protein inhibitor (FAPI)-PET/CT. B cell depletion was quantified in blood, synovium, and lymph nodes.
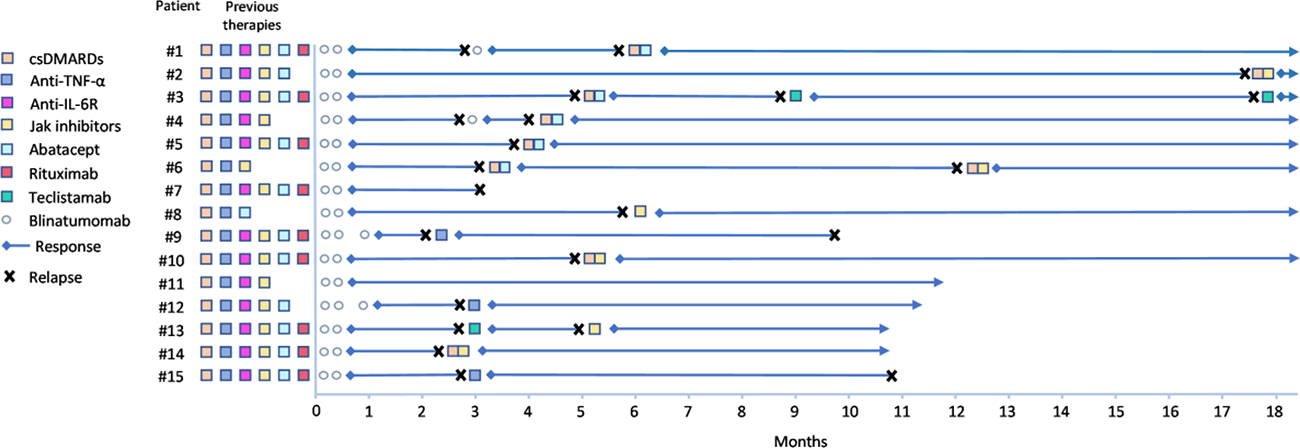
Results: Blinatumomab was safe. No ICANS or hypogammaglobulinemia occurred. Three cases of grade 1 CRS (#9, #13, #14) were reported. Blinatumomab induced short B cell aplasia in the peripheral blood. B cells were also depleted in the synovium (4/5 biopsies) but not in the lymph nodes. Rapid clinical response was observed in all patients. At month 3, the median number of tender joints had decreased from 9 [range: 2–39] to 2 [range: 0–23], the number of swollen joints from 8 [range: 1–35] to 1 [range: 0–12] and VAS had improved from 70 [range: 40–100] to 35 [range: 0–90]. Correspondingly, DAS28-CRP decreased from 4.8 to 2.4. Hence, all 15 patients reached at least ACR20 response criteria, 73% (11/15) reached at least an ACR50 response, 53% reached at least an ACR70 response and 33% (5/15) reached DAS28-CRP remission by month 3. Fibroblast activation tended to decrease, most notably in large joints. However, clinical effects of blinatumomab were not sustained. RA relapse occurred in 93% (14/15) of patients, requiring re-initiation of immunosuppressive therapy. At relapse, five patients (#1, #3, #4, #5, #6) received abatacept and remission or at least low disease activity (LDA) was restored even in patients who previously failed on abatacept. Two of these patients (#3, #6) lost abatacept responses later and were then switched to the BCMA -T cell engager teclistamab (#3), and Janus kinase (JAK) inhibitor upadacitinib (#6) regaining remission. JAK inhibitors were introduced in a total of five patients (#2, #6, #8, #10, #14), including the one patient cycling through abatacept. All five patients achieved LDA or remission. Notably, four of these patients had previously failed on JAK inhibitors, again indicating a restoration of therapeutic sensitivity. Three additional patients (#9, #12, #15) were treated with TNF-alpha inhibitors (#9 infliximab, #12 etanercept, #15 adalimumab) upon relapse. All of them had previously failed on anti-TNF. Re-treatment with TNF-inhibitors after blinatumomab led to LDA in patient #12. Although DAS28-CRP decreased also in patient #9 and #15, it remained persistently > 4 in both patients. One additional patient relapsing (#13) was also treated with the BCMA T cell engager teclistamab, initially reaching LDA but relapsing again and then reaching low LDA with the JAK inhibitor filgotinib. Overall blinatumomab treatment restored responsiveness to previously failed therapies in most patients (Figure 1).
Conclusions: At low TCE doses, incomplete B-cell depletion within lymph nodes likely precludes a curative immune reset. Nevertheless, low-dose blinatumomab reduced fibroblast activation and restored responsiveness to DMARDs that extended beyond the treatment period. We propose that this “immune dimming” serves as a pragmatic alternative to full “immune reset,” offering a feasible dosing strategy that effectively breaks the cycle of treatment resistance.
Table 1. Baseline characteristics of patients treated with blinatumomab, stratified by disease activity (DAS 28 CRP).
Clinical course after blinatumomab and the re-introduction of previous therapies at relapse.
REFERENCES: [1] Bucci L, Hagen M et al. Nat Med. Jun 2024;30(6):1593-1601.
[2] Ruck T, Huntemann N, et al. Mol Ther. Sep 3 2025;33(9):4135-4142.
[3] Subklewe M, Magno G, et al. Eur J Cancer. Jun 2024;204:114071.
Acknowledgments: NIL.
Disclosure of Interests: Laura Bucci: None declared, Melanie Hagen: None declared, Sebastian Boeltz: None declared, Carlo Tur: None declared, Danae-Mona Nöthling: None declared, Tobias Dashi: None declared, Janina Auth: None declared, Tobias Rothe: None declared, Andreas Wirsching: None declared, Jochen Wacker: None declared, Andrea Zoli: None declared, Anna-Maria Liphardt: None declared, Stefano Alivernini: None declared, Luis Munoz: None declared, Verena Schönau: None declared, Jürgen Rech: None declared, Armin Atzinger: None declared, Maria Antonietta D’ Agostino Abbvie, Amgen, Novartis, BMS, UCB, J&J, Biogen, MSD, Lilly and Galapagos, Amgen, Abbvie, UCB, Pfizer, J&J and Galapagos, Aline Bozec: None declared, Markus Eckstein: None declared, Maria Gabriella Raimondo: None declared, Georg Schett BMS, Cabaletta, Janssen, Kyverna, Miltenyi, and Novartis, Ricardo Grieshaber-Bouyer AbbVie, Alfasigma, AstraZeneca, Bristol-Myers Squibb, Candid Therapeutics, Cullinan Therapeutics, Epana Bio, Gilead, Kite, Johnson & Johnson, Kyverna Therapeutics, Lilly, Novartis, Pfizer, Sanofi, Xencor, UCB.