fetching data ... 
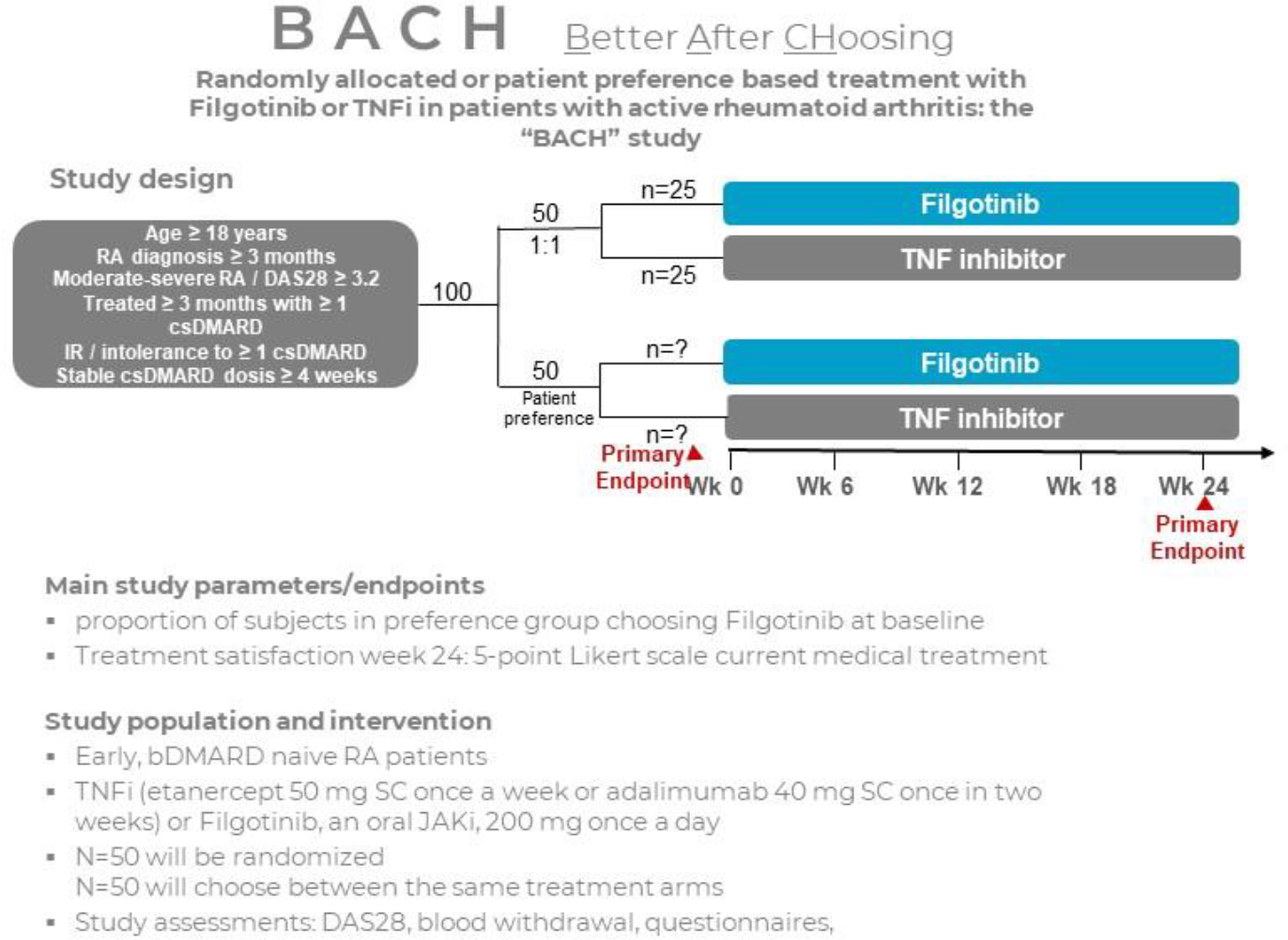
Background: The use of Shared Decision Making (SDM) in the treatment of Rheumatoid Arthritis (RA) improves patients’ self-management and their engagement in their treatment. A better adherence and higher treatment satisfaction has been shown for patients with RA who engaged in SDM for biological (b)DMARD treatment selection. While the value of SDM in the treatment of RA is increasingly evident, there is still limited evidence on the extent to which RA patients are able to act autonomously when choosing their own treatment and what the impact of patients choosing is on clinical outcomes and patient experience. We evaluated the treatment preference and treatment satisfaction of patients with active RA when they were given the opportunity to personally choose the subsequent mode of action for their medication after failure of treatment with conventional (cs)dmards. We hypothesised patient choice to have a positive effect on treatment satisfaction and designed a strategic study; not to compare two treatment modalities but to establish the influence of patient participation on treatment satisfaction and disease activity (Treat by Choice; tbc). We conducted a randomised trial for bdmard naive RA patients, designed to evaluate the treatment preference of RA patients when invited to personally choose between treatment with the oral Janus Kinase Inhibitor (jaki) filgotinib or a subcutaneous (SC) Tumor Necrosis Factor inhibitor (tnfi) and to compare treatment satisfaction between patients who are able to choose their own treatment and patients who are randomised to these same treatment options, as is shown in figure 1.
Objectives: Primary Objective for the Choice Group N=50: to evaluate the actual preference of RA patients when they decide which mode of action they want to use for treatment of their RA after treatment with conventional dmards failed. Primary objective for the total study population N=100 (Choice Group versus the randomisation group): to evaluate the difference in treatment satisfaction between patients who chose their own therapy and patients that were randomised to the same treatment options. Main secondary objective: to evaluate the difference in improvement of disease activity by the Disease Activity Score (DAS28) between the choice and randomisation groups.
Methods: We conducted an unblinded, open label, parallel group, investigator-initiated, multicenter, phase IV trial in The Netherlands, with a 24 week treatment period, designed to evaluate the treatment preference of RA patients, when they are invited to personally choose between treatment with the oral jaki filgotinib or SC tnfi. The study also compares treatment satisfaction between patients who are able to choose their own treatment and patients who are randomised to these same treatment options. Patients with moderate to severe active RA, defined as a Disease Activity Score (DAS)28 ≥ 3.2 or at the discretion of the treating rheumatologist and who failed to reach remission on csdmards, were randomised 1:1 to either personally choose between SC tnfi or oral jaki filgotinib; or to be randomised to the same treatment options. To maintain the neutrality of the healthcare providers in the process of choosing, the subjects randomised to the open choice group were then informed by a standardised, neutral information video. Potential questions would be answered by predefined frequently asked questions (FAQ’s). All participants received regular care and followed an identical visit schedule and completed the same study procedures. At each visit, a DAS28 score was obtained and treatment satisfaction was measured on a 5 point Likert scale. Methotrexate and prednisone dosages were pragmatically tapered wherever possible. Patients who demonstrated insufficient clinical improvement were managed according to standard rheumatological care and were allowed to switch to the other mode-of-action therapy after week 12. They were censured in the results for DAS28 as “treatment switchers”. The use of non-steroidal anti-inflammatory drugs (nsaids) and paracetamol/acetaminophen as rescue medication was allowed and initiation of corticosteroids was left to the discretion of the treating rheumatologist. During the study, the exclusion criteria were sharpened according to an EMA advice on all jaki for potential risk categories.
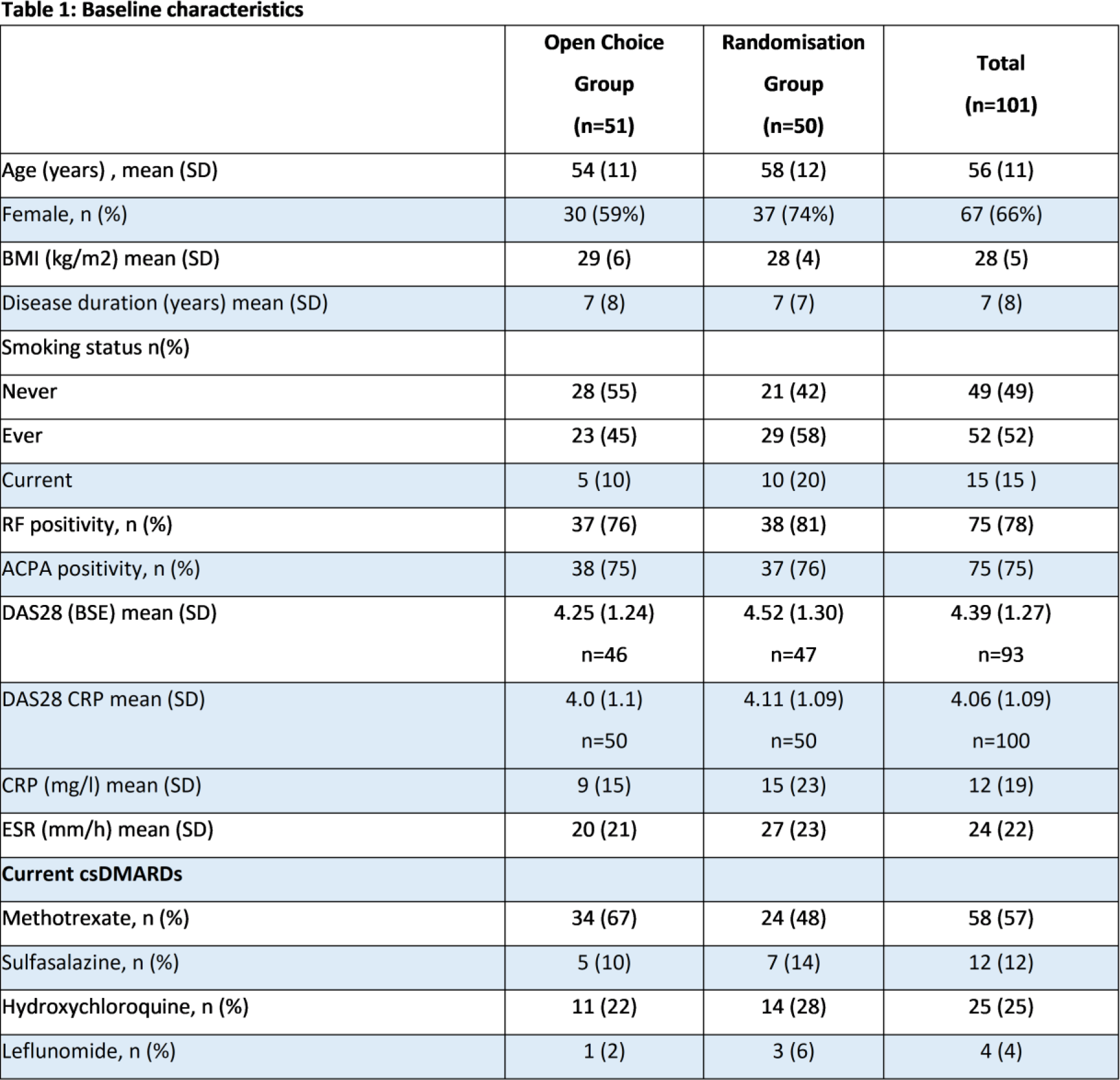
Results: Table 1 shows the baseline characteristics of the two patient groups. All patients in the open choice group were able to make their treatment choice within 48 hours. In the open choice group, patients preferred oral jaki; 55% (n=28) versus 45% (n=23) for subcutaneous tnfi. Treatment satisfaction at week 24 was significantly higher in the open choice group, compared to the randomisation group (46 vs 33, p=0.012), regardless of the type of treatment they either chose or were randomised to. By week 12, fewer patients in the open choice group than in the randomisation group switched to a different mode of action (6 vs 15, p=0.026), this was primarily due to persistent disease activity. At week 24, the mean DAS28-ESR was numerically, although not significantly, lower in the open choice group (2.24 vs 2.71, p=0.083). In the randomised group, more corticosteroids were being used at the end of the study (week 24:4 vs 12 patients, p=0.031). The number of adverse events per patient was significantly higher in the randomisation group (1.61 versus 2.02, p=0.046).
Conclusions: Our findings demonstrate that patients with rheumatoid arthritis are capable of making treatment decisions without hesitation. When given the opportunity to choose, patients with active RA prefer oral jaki over subcutaneous injections tnfi. Patients who choose their own treatment have significantly higher treatment satisfaction, better drug retention and report less adverse events. Treat by Choice should be considered as a valuable treatment strategy in daily clinical practice.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Floor Reimann: None declared, Nic Veeger: None declared, Annemiek Willemze: None declared, Floris A. Van Gaalen grants and/or fees from: abbvie, Assessment of spondyloarthritis international Society, BMS, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB (all paid to employer)., letty versteeg: None declared, rens besseling: None declared, inge klein-wieringa: None declared, freke wink: None declared, lidy hendriks: None declared, annemarie schilder: None declared, tjitske berends-de vries: None declared, dan zhang: None declared, Harald E. Vonkeman Abbvie, Novartis, Pfizer, UCB, Lilly, astrazeneca, Alfasigma, Boehringer Ingelheim, Johnson and Johnson, Alfasigma; DSMB: Alfasigma, Galapagos and Boehringer Ingelheim,, Tom Huizinga research support/lecture fees/consultancy fees from Brystol Myers Squibb, Janssen, Pfizer, Novartis, and Eli Lilly, research support/lecture fees/consultancy fees from Brystol Myers Squibb, Janssen, Pfizer, Novartis, and Eli Lilly, The grant from Alfasigma for sponsoring of this trial, reinhard bos Johnson & Johnson, Abbvie, Alfasigma, Johnson & Johnson, funding/grant for investigator initiated research in this study: BACH: started by Galapagos, continued by Alfasigma.