fetching data ... 
Background: Previous studies indicate an uncoupling between pain and inflammation during the disease course in a substantial proportion of rheumatoid arthritis (RA) patients, with significant unresolved pain despite inflammation control [1,2]. Development of a non-nociceptive pain state through peripheral and/or central sensitisation has attained increased focus as a potential cause, but it remains unclear whether this is due to a prolonged period of insufficiently controlled inflammation early in the disease.
Objectives: To investigate whether failure to reach remission during the first 24 weeks is linked to more non-inflammatory pain features at 48 weeks compared to early as well as versus later remission attainment, in aggressively treated new-onset RA patients without concomitant chronic widespread pain at treatment start.
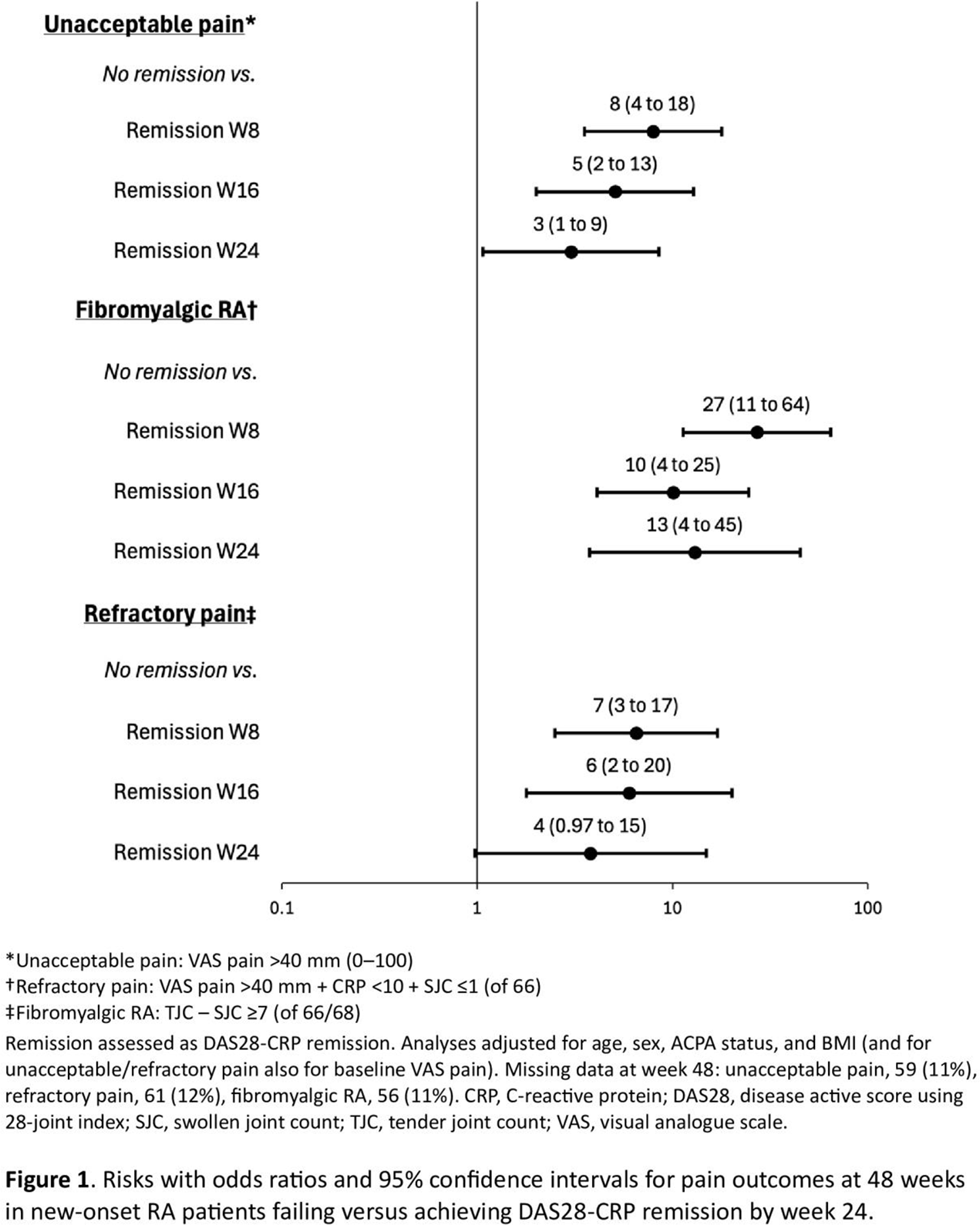
Methods: In the investigator-initiated, open-label NORD-STAR trial, patients with early (<2 years) RA were randomised to methotrexate combined with (a) other csDMARDs/corticosteroids or corticosteroids alone (tapered in 9 weeks), (b) certolizumab pegol, (c) abatacept, or (d) tocilizumab [3,4]. Having a chronic widespread pain condition was an exclusion criterium of NORD-STAR and such patients hence not part of the present analyses. Additionally, the tocilizumab arm was omitted due to its selective effect on CRP which was included as a component in one of the composite pain measures. Patients were otherwise analysed irrespective of randomised therapy. The exposure was: time to first DAS28-CRP remission (at 8, 16, or 24 weeks) or no remission during the first 24-week period. 48-week pain outcomes were defined as: (A) Unacceptable pain (visual analogue scale [VAS] pain>40 mm [0–100]) [5], (B) Refractory pain (unacceptable pain + CRP<10 mg/L + swollen joint count [SJC]≤1 [of 66]) [1], and (C) Fibromyalgic RA (tender joint count [TJC] – SJC ≥7 [here modified to be calculated from the 66/68-joint index]) [6]. Associations between time to first DAS28-CRP remission and pain outcomes were analysed with logistic regression and adjusted for age, sex, ACPA positivity, and BMI. Additional adjustment for baseline VAS pain was conducted for pain outcomes where VAS pain was a constituent (unacceptable pain and refractory pain).
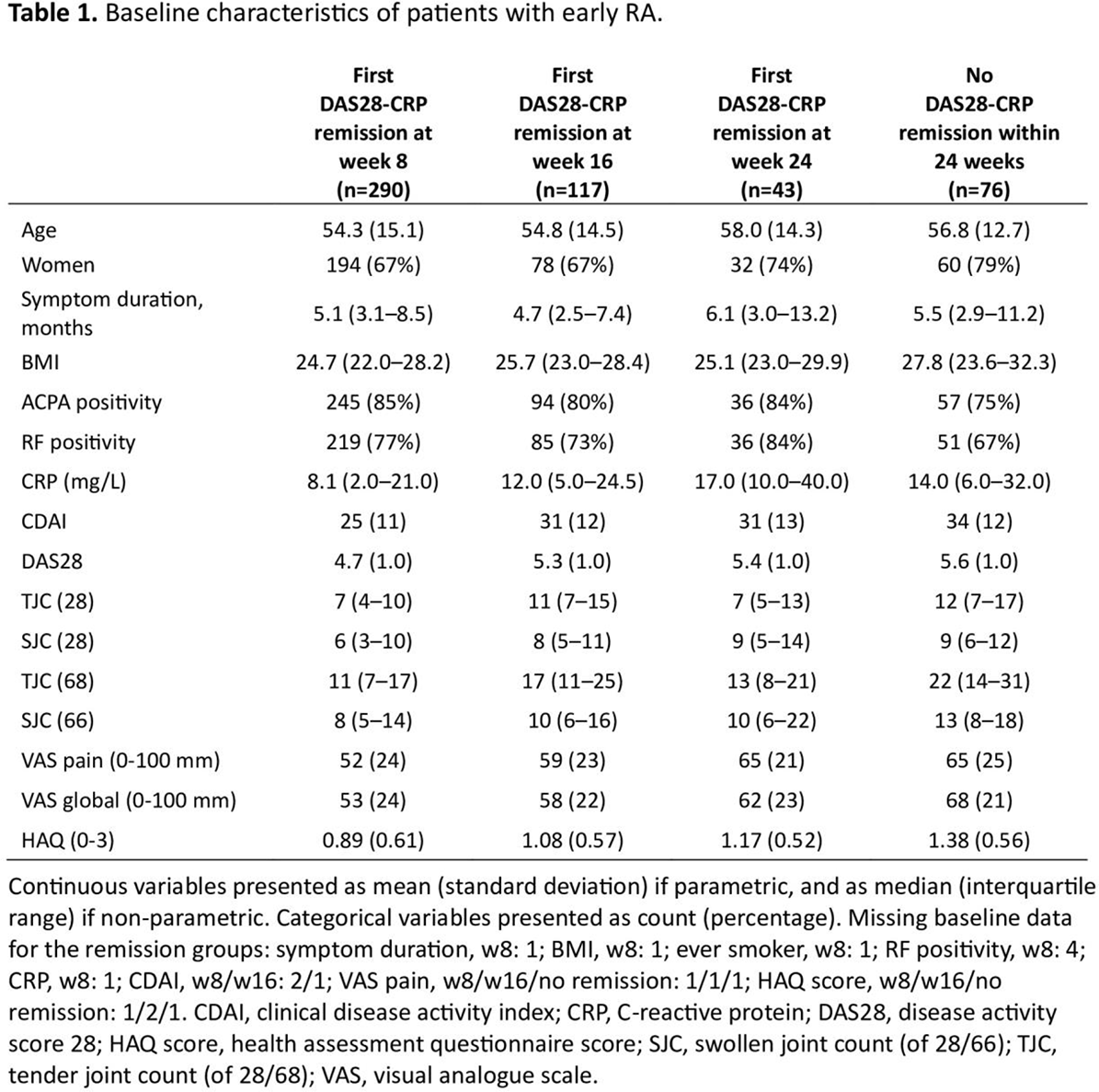
Results: Out of 526 patients with available data for assessment of first DAS28-CRP remission at the studied follow-up time-points, 450 achieved remission within 24 weeks (at week 8, 16 or 24), whereas 76 patients did not. The baseline characteristics are shown in Table 1 . Patients without remission during the first 24 weeks were significantly more likely to have unacceptable pain at 48 weeks than remission achievers (adjusted OR 6.2 [95%CI 3.1-12.4]), with larger estimates when comparing no remission with early remission (adjusted OR 7.9 [95%CI 3.5-17.8] vs. remission week 8) than when comparing no remission with later remission (adjusted OR 3.0 [95%CI 1.1-8.5] vs. remission week 24) ( Figure 1 ). Patients not reaching remission within 24 weeks also had significantly more refractory pain at week 48 than remission achievers (adjusted OR 6.2 [95%CI 2.7-14.3]), also here with larger estimates when comparing no remission with early remission (adjusted OR 6.5 [95%CI 2.5-16.9] vs. remission week 8) than when comparing no remission with later remission (adjusted OR 3.8 [95%CI 1.0-14.8] vs. remission week 24). Fibromyalgic RA at week 48 was likewise more frequent among patients who failed to reach remission during the first 24 weeks compared to remission achievers (adjusted OR 16.3 [8.0-32.8]), again with greater estimates when comparing no remission with early remission (adjusted OR 27.0 [95%CI 11.3-64.5] vs. remission week 8) than when comparing no remission with later remission (adjusted OR 13.0 [95%CRI 3.8-45.1] vs. remission week 24).
Conclusions: Newly diagnosed RA patients without a previous chronic widespread pain condition, who fail to reach remission within 24 weeks of aggressive anti-rheumatic treatment, were more likely to have non-inflammatory pain at 48 weeks than remission achievers. The difference was most marked when comparing with patients achieving very early remission at week 8, supporting an association between initially sustained inflammatory load and subsequent non-inflammatory pain [2], and underscoring the importance of early aggressive treatment.
REFERENCES: [1] Olofsson et al. Arthritis Care Res 2021;73:1312-21.
[2] Brink et al. Arthritis Rheumatol 2025;77 (Suppl 9).
[3] Hetland et al. BMJ 2020;2;371:m4328.
[4] Østergaard et al. Ann Rheum Dis 2023;82:1286-95.
[5] Tubach et al. Arthritis Care Res 2012;64:1699-72.
[6] Pollard et al. Rheumatology 2010;49:924-28.
Jon Lampa and Tor Olofsson contributed equally
Acknowledgments: NIL.
Disclosure of Interests: Annie Brink: None declared, Johan K Wallman AbbVie, Amgen, Eli Lilly, Novartis, Pfizer, Hilde Berner Hammer AbbVie, Eli Lilly, Novartis and UCB, Jon T Einarsson: None declared, Meliha C Kapetanovic: None declared, Elisabeth Mogard AbbVie, Elisabet Lindqvist: None declared, Carmen Roseman: None declared, Kristina Lend: None declared, Merete Lund Hetland Sandoz, UCB, Norvartis, AbbVie, Alfasigma, AbbVie, Eli Lilly, Sandoz, UCB, Novartis, Mikkel Østergaard Abbvie, BMS, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, MEDAC, Merck, Novartis, Pfizer, UCB, Abbvie, AlfaSigma, BMS, Celgene, Eli Lilly, Galapagos, Gilead, Janssen, Merck, Novartis, Pfizer, UCB, AbbVie, Amgen, BMS, Celgene, Eli Lilly, Merck, Novartis, UCB, Kim Hørslev-Petersen: None declared, Dan Nordström AbbVie, Lilly, MSD, Novartis, Pfizer, UCB, Tuulikki Sokka-Isler: None declared, Bjorn Gudbjornsson: None declared, Gerdur Grondal: None declared, Marte S Heiberg: None declared, Espen A. Haavardsholm: None declared, Mike Nurmohamed: None declared, Anna Rudin: None declared, Ronald F. van Vollenhoven AbbVie, AstraZeneca, Biogen, BMS, Cabaletta, Galapagos, GSK, Janssen, Kyowakirin, Pfizer, RemeGen, Sanofi, UCB, Vorbio, AbbVie, AstraZeneca, Biogen, BMS, Cabaletta, Galapagos, GSK, Janssen, Kyowakirin, Pfizer, RemeGen, Sanofi, UCB, Vorbio, Alfasigma, AstraZeneca, BMS, Cabaletta, Galapagos, MSD, Novartis, Pfizer, RemeGen, Roche, Sanofi, UCB, Till Uhlig: None declared, Jon Lampa: None declared, Tor Olofsson: None declared.