fetching data ... 
Background: Current EULAR [1] and ACR [2] gout guidelines recommend lifelong urate−lowering therapy (ULT) using a treat−to−target (T2T) strategy to maintain remission in gout patients. However, evidence of superiority of a continued T2T ULT strategy over a ULT discontinuation attempt strategy during remission is lacking. In addition, adherence to ULT is often poor and discontinuation common.
Objectives: To assess whether a continued T2T ULT strategy is superior to a ULT discontinuation attempt strategy in maintaining gout remission.
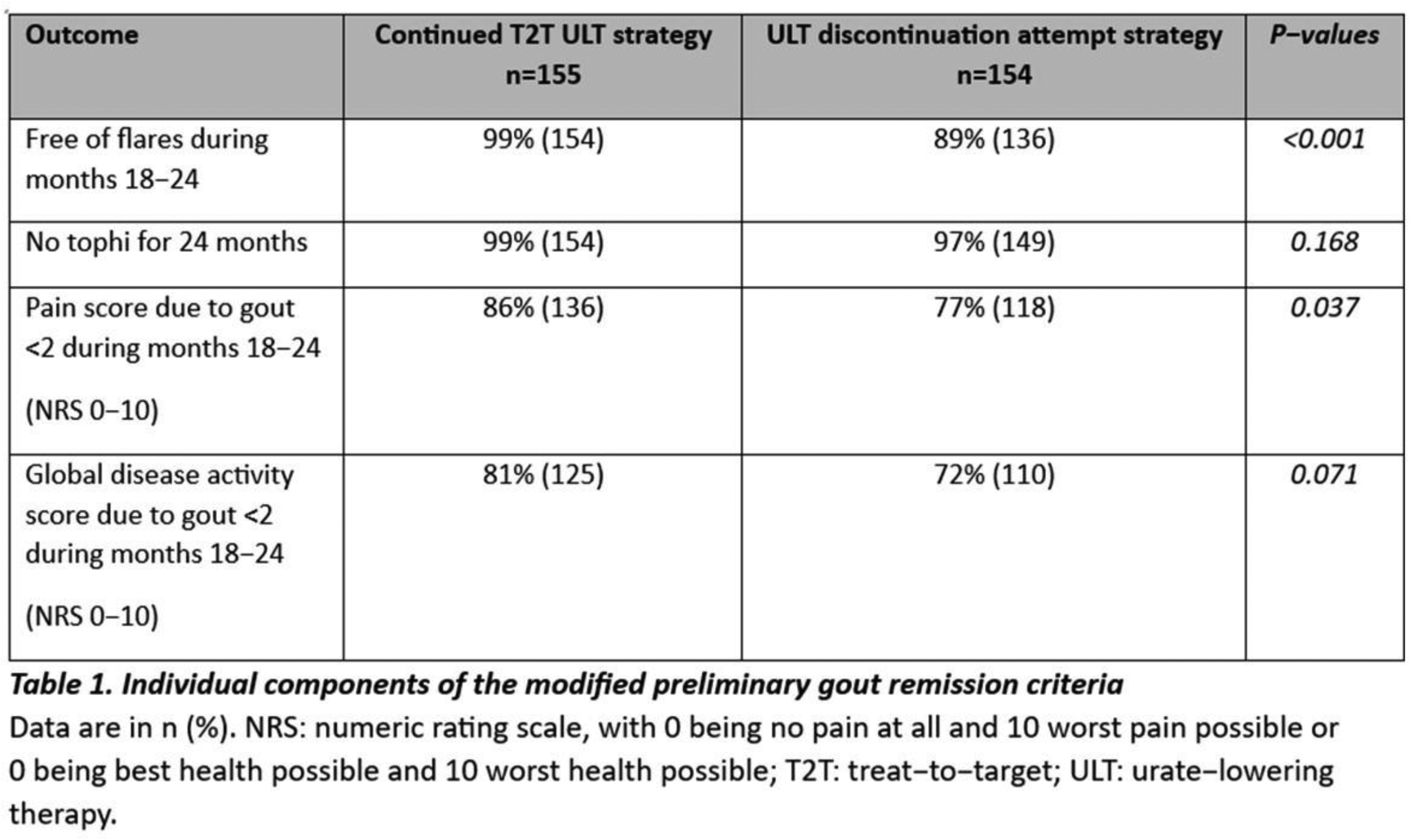
Methods: An open-label, pragmatic, multicentre, randomised superiority trial across nine rheumatology clinics in the Netherlands was conducted. Adult patients with gout who had been in remission for ≥12 months while using ULT (allopurinol, benzbromarone and/or febuxostat) were eligible. Remission was defined as serum urate <0.36 mmol/L, absence of tophi, no gout flares, gout pain score <2 (0-10), and patient global disease activity <2 (0-10). Patients were randomised using centralised computer-generated allocation 1:1 to continued T2T ULT or a ULT discontinuation attempt, with protocolised restart in case of recurrent flares or tophus development. Follow-up duration was 24 months. The primary outcome was the difference in proportion of patients in remission during the final six months of follow-up between both strategies, assessed using modified preliminary gout remission criteria (free of flares during months 18−24, no tophi during 24 months, gout pain score <2 (0-10) and patient global disease activity <2 (0-10)). Missing components of the primary outcome were imputed using multiple imputation by chained equation forming 20 imputed datasets. Additionally a complete-case analysis was performed, as well as a post−hoc analysis using simplified gout remission criteria (without serum urate and patient reported outcomes). Secondary outcomes were time to loss of flare−free status over 24 months, serum urate levels, ULT restart, use of anti-inflammatory medication, adverse events with special interest in major cardiovascular events and change in kidney function. Analyses were performed according to the intention-to-treat principle.
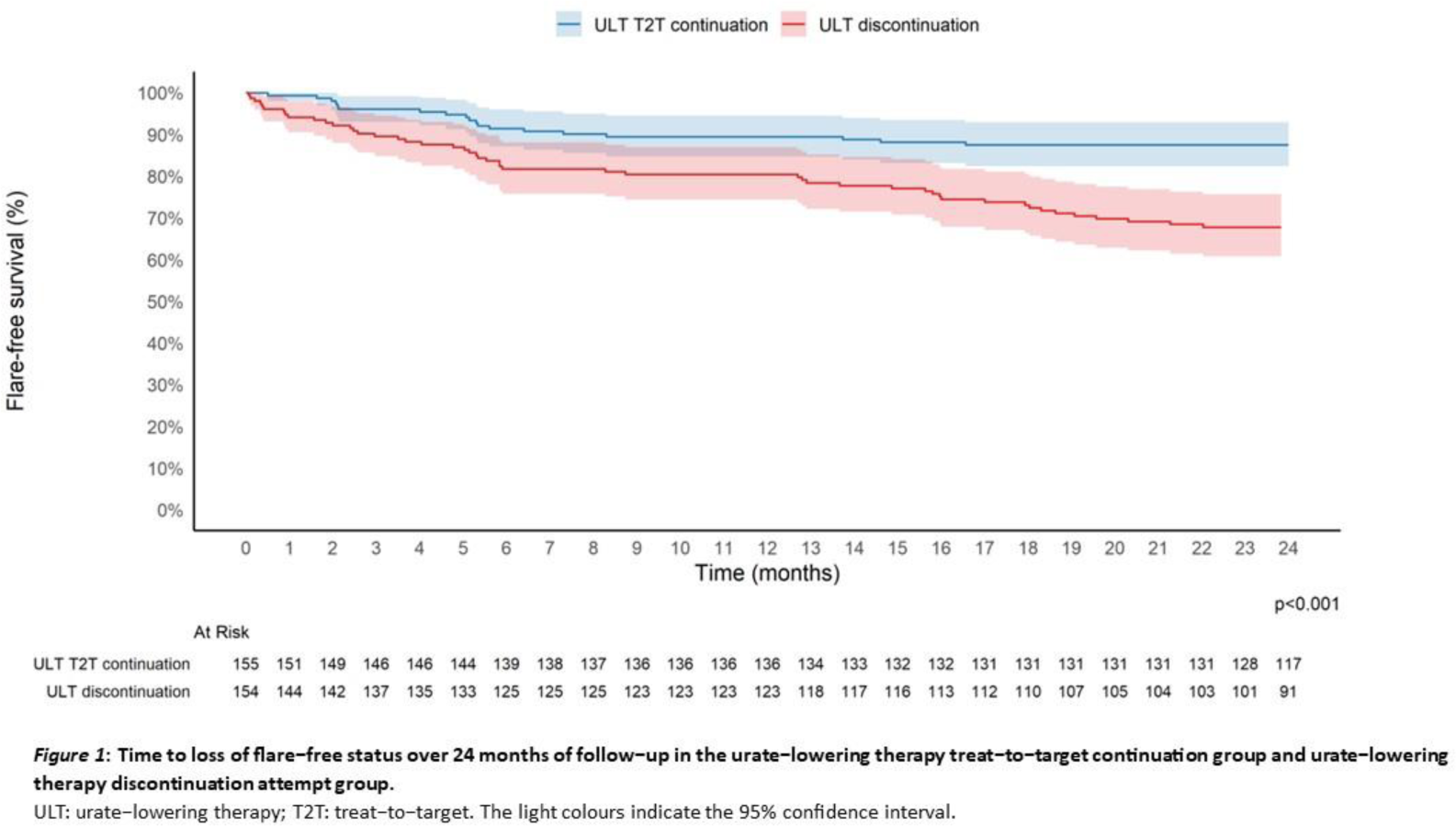
Results: Between February 2021 and June 2023, 309 participants were randomised (155 to ULT continuation and 154 to ULT discontinuation). Median age was 68 years (60-73), 94% were male, 90% were using allopurinol at baseline and mean serum urate concentration at baseline was 0.28mmol/L (SD 0.05). Primary outcome components were missing in 6.5%. Remission criteria during the final six months of follow−up were met in 79.2% (123/155) of participants in the continued T2T ULT group compared with 62.9% (97/154) in the ULT discontinuation attempt group (risk difference (RD) 16.3%; 95% CI 6.1% to 26.5%; p=0.002). Individual remission components are shown in Table 1. Complete-case analysis (only those with all remission components available) showed similar results (81% vs 63%; RD 18%; 95% CI 8% to 27%; p<0.001). Time to loss of flare−free status over 24 months was higher with ULT continuation, with a cumulative flare incidence of 12.3% (9.7 per 100 person-years; 95% CI, 6.7 to 13.9) compared with 31.8% (28.4 per 100 person-years; 95% CI 23.0 to 35.0) in the ULT discontinuation attempt group (incidence rate ratio, 0.34; 95% CI 0.22 to 0.52). Flare-free survival curves are shown in Figure 1. Mean serum urate increased 2 weeks after ULT discontinuation to 0.46 mmol/L (SD 0.09) and remained elevated at 12 and 24 months, whereas it remained stable in the T2T ULT continuation group 0.28 mmol/L (SD 0.06) at 12 months and 0.29 mmol/L (SD 0.07) at 24 months). In the ULT discontinuation group, 23% of participants restarted ULT after a median of 392 days (interquartile range 238 to 603). Use of any anti−inflammatory medication occurred in 18% of participants in the continued T2T ULT group compared with 36% in the ULT discontinuation attempt group (RD −18%; 95% CI −27% to −8%; p<0.001). A total of 73 adverse events occurred in 46 participants in the continued T2T ULT group, compared with 122 events in 75 participants in the ULT discontinuation attempt group. This corresponds to cumulative incidences of respectively 30% (46/155) and 49% (75/154) (RD −19%; 95% CI −30% to −8%; p<0.001), with arthralgia more frequently reported after ULT discontinuation. Major cardiovascular events occurred 12 times in the T2T ULT group and 10 times in the ULT discontinuation attempt group and in both groups 3 deaths occurred (heart failure n=1, cardiac arrest n=1, trauma n=2 and malignancy n=2). Mean CKD-EPI at 24 months was significantly lower in the ULT discontinuation attempt group than in the continued ULT T2T group (ANCOVA baseline adjusted mean difference −1.84 mL/min/1.73 m 2 ; 95% CI −3.52 to −0.15; p=0.033). In a post-hoc analysis using simplified gout remission criteria (without serum urate and patient reported outcomes), remission rates were higher in both groups, with 98.6% (153/155) in the continued T2T ULT group and 86.4% (133/154) in the ULT discontinuation attempt group (RD 12.2%; 95% CI 6.3 to 18.1; p<0.001).
Conclusions: Over a two-year follow-up period, a continued T2T ULT strategy resulted in higher rates of gout remission during the final six months compared with a ULT discontinuation attempt strategy and resulted in fewer flares and less anti-inflammatory medication use. These findings support current guideline recommendations to continue ULT during remission and inform shared decision-making discussions about whether to (dis)continue ULT. The modest kidney function benefit observed further supports routine ULT continuation during remission. However, a substantial proportion of patients remained flare-free after ULT discontinuation. Future research should study more long-term outcomes and safety, define predictors of (un)successful discontinuation and assess cost-effectiveness.
REFERENCES: [1] Richette P, et al. Ann Rheum Dis . 2017;76:29-42.
[2] FitzGerald JD, et al. Arthritis Care Res . 2020;72:744-60.
Acknowledgments: NIL.
Disclosure of Interests: Iris Rose Peeters: None declared, A.A. den Broeder: None declared, Maike H.M. Wientjes: None declared, Nathan den Broeder N. den Broeder has received research grants from AbbVie, Galapagos, Lilly, Johnson and Johnson, Pfizer, UCB and Novartis, Amy C D Peeters: None declared, Leo Joosten: None declared, Debby den Uyl: None declared, Tim Jansen: None declared, Marijn Smits: None declared, Lenny van Bon L. van Bon has received a grant from FOREUM., Pascal H.P. de Jong: None declared, Harald E. Vonkeman H.E. Vonkeman is a paid consultant for Abbvie, Novartis, Pfizer, UCB, Johnson and Johnson and Alphasigma, H.E. Vonkeman has received speaker fees from AstraZeneca, Lilly, Pfizer and Alphasigma., H.E. Vonkeman has received research grants from Galapagos and Boehringr Ingelheim., Marie-Luise Oudemans: None declared, William Taylor: None declared, Caroline van Durme: None declared, Wing-Yee Kwok: None declared, Henk J Schers: None declared, Marcel Flendrie: None declared, Noortje van Herwaarden: None declared.